Identifying and Managing CAR T-Associated Hemophagocytic Lymphohistiocytosis Following Dual-Targeted CAR T-Cell Therapy
Presentation
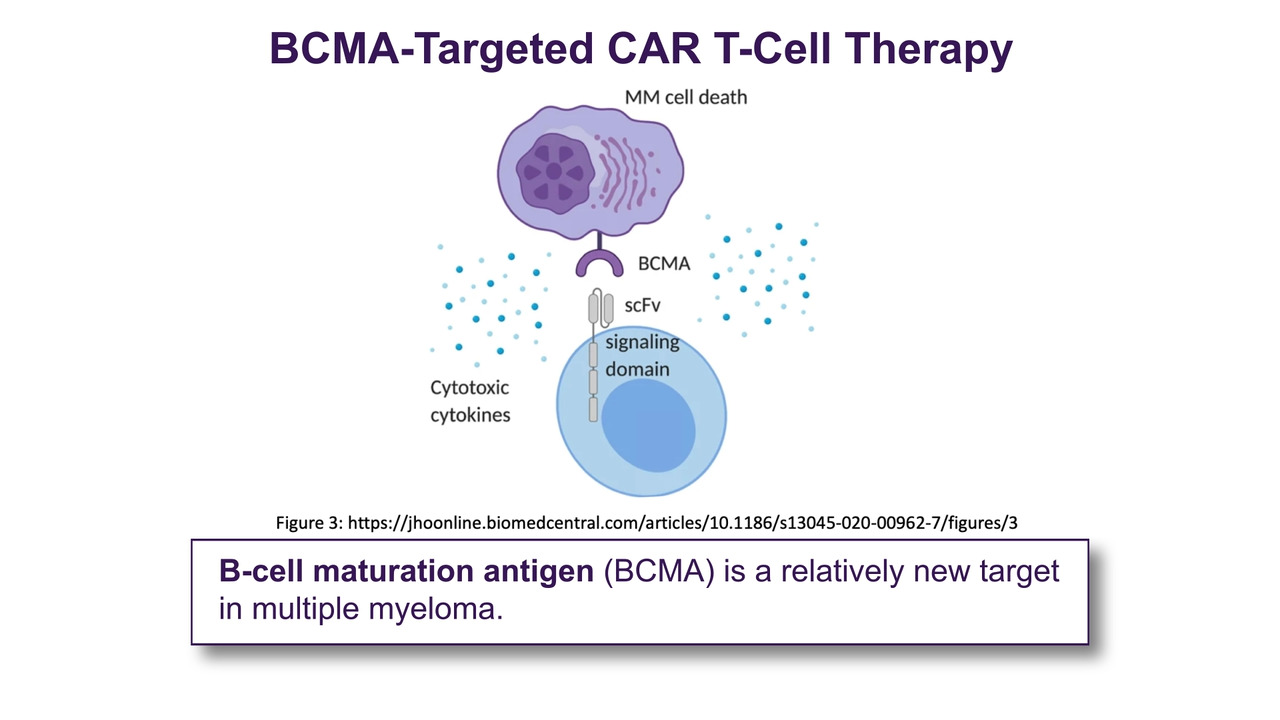
A 43-year-old female with relapsed/refractory multiple myeloma was admitted for participation in a CD19xBCMA–directed CAR T-cell clinical trial after disease progression through 5 prior lines of therapy, including:
- VRd (bortezomib, lenalidomide, dexamethasone)
- bPD (pomalidomide, bortezomib, dexamethasone)
- Autologous stem cell transplant
- DKd (daratumumab, carfilzomib, dexamethasone)
- DKCd (daratumumab, carfilzomib, cyclophosphamide, dexamethasone)
She underwent standard lymphodepleting chemotherapy prior to CAR T-cell infusion. Her initial post-infusion course was uneventful until Day +11, when she developed fever and hypoxia requiring 3L oxygen via nasal cannula.
Workup, Diagnosis, and Treatment
Day +11
The patient’s vital signs were notable for:
- Temperature: 102.1°F
- Blood pressure: 102/64 mm Hg
- Heart rate: 118 beats per minute
- Respiratory rate: 24 breaths per minute
- Peripheral capillary oxygen saturation: 89% on room air, improved to 95% on 3L nasal cannula
An infectious workup was initiated, including blood cultures, chest imaging, and viral studies. Initial evaluation was unrevealing.
The patient met criteria for grade 2 cytokine release syndrome (CRS) due to fever and oxygen requirement. She received 8 mg/kg of intravenous tocilizumab and 10 mg of intravenous dexamethasone. Due to persistent fever and hypoxia 12 hours later, repeat dosing of tocilizumab and dexamethasone was administered.
By Day +12, her fever and oxygen requirements resolved.
Day +13
Laboratory evaluation demonstrated rapidly worsening inflammatory markers and progressive organ dysfunction:
- Ferritin: >37,500 ng/mL
- Lactate dehydrogenase (LDH): 1,940 U/L
- Triglycerides: 394 mg/dL
- Alkaline phosphatase: 424 U/L
- Alanine aminotransferase (ALT): 362 U/L
- Aspartate aminotransferase (AST): 398 U/L
- Total bilirubin: 1.1 mg/dL
- Persistent pancytopenia despite count recovery window
Given concern for immune effector cell-associated hemophagocytic lymphohistiocytosis (IEC-HS/HLH), additional workup was initiated, including soluble CD25 level, cytokine panel, Epstein-Barr virus polymerase chain reaction (PCR), cytomegalovirus PCR, and abdominal ultrasound.
Per American Society for Transplantation and Cellular Therapy (ASTCT) grading criteria, the patient had grade 2 HLH. Per ASTCT recommendations for management of CAR T-associated HLH, the patient was started on anakinra 100 mg subcutaneously twice daily and intravenous dexamethasone 10 mg daily.
Day +13 (later evaluation)
Despite initiation of therapy, inflammatory markers and liver function tests worsened over the next 24 hours:
- Ferritin: >37,500 ng/mL
- LDH: 3,487 U/L
- Triglycerides: 416 mg/dL
- ALT: 432 U/L
- AST: 455 U/L
- Alkaline phosphatase: 501 U/L
- Total bilirubin: 2.8 mg/dL
Given concern for refractory and evolving HLH-like toxicity, anakinra was escalated to 200 mg every 6 hours.
Day +14
Repeat laboratory studies demonstrated partial improvement but ongoing evidence of severe systemic inflammation:
- Ferritin: 34,005 ng/mL
- LDH: 2,787 U/L
- Triglycerides: 411 mg/dL
- ALT: 288 U/L
- AST: 263 U/L
- Alkaline phosphatase: 368 U/L
- Total bilirubin: 2.6 mg/dL
- Persistent cytopenias
Due to ongoing concern for active IEC-HS/HLH, 10 mg oral ruxolitinib twice daily was initiated. Anakinra and dexamethasone were continued.
Day +18
Inflammatory markers, liver enzymes, and cytopenias began to improve. Oxygenation remained stable, and no recurrent CRS symptoms developed. Given clinical improvement, dexamethasone, anakinra, and ruxolitinib were gradually tapered.
Day +28
By Day +28, the patient’s ferritin had normalized, liver function tests had normalized, cytopenias improved, and inflammatory markers had resolved. The patient was discharged from the hospital in stable condition. A bone marrow biopsy demonstrated a very good partial response.
Discussion
IEC-HS, also referred to as CAR T-associated HLH-like toxicity, is a rare but potentially life-threatening hyperinflammatory syndrome that can occur following CAR T-cell therapy.
Clinical manifestations often overlap with CRS and may include marked hyperferritinemia, refractory cytopenias, hepatic dysfunction, coagulopathy, hypertriglyceridemia, elevated LDH, and/or persistent fevers despite CRS-directed therapy.
IEC-HS most commonly develops after or concurrent with CRS resolution and is thought to result from uncontrolled immune activation and macrophage hyperactivation. Distinguishing HLH from prolonged CRS or infection can be clinically challenging.
In 2023, the ASTCT published consensus recommendations for the diagnosis and management of IEC-HS following immune effector cell therapy.1 Suggested management strategies include corticosteroids and cytokine-directed therapies such as anakinra, with escalation to additional immunomodulatory agents including ruxolitinib in patients with refractory disease.
In this case, the patient demonstrated progressive hyperinflammation despite initial corticosteroid and anakinra therapy, requiring escalation to high-dose anakinra and subsequent addition of ruxolitinib. Following multimodal immunosuppressive therapy, laboratory abnormalities and clinical symptoms gradually resolved without apparent compromise of antimyeloma response.
This case highlights the importance of early recognition of evolving HLH-like toxicity, serial monitoring of ferritin and liver function tests after CRS, prompt escalation of immunosuppressive therapy when inflammatory markers worsen, and the use of ASTCT guidance to support management decisions in severe IEC-HS.
Clinical Pearls
IEC-HS/HLH is a rare but serious complication following CAR T-cell therapy. Clinical features such as hyperferritinemia, worsening cytopenias, transaminitis, and hypertriglyceridemia following CRS should raise concern for HLH, even in patients with improving CRS symptoms. Anakinra is increasingly used as frontline therapy for CAR T-associated HLH, whereas ruxolitinib may be considered in patients with refractory or progressive disease. Early recognition and treatment are critical to preventing multiorgan dysfunction.
Reference
- Hines MR, Keenan C, Maron Alfaro G, et al. Immune Effector Cell-Associated Hemophagocytic Lymphohistiocytosis-like Syndrome (IEC-HS). Transplant Cell Ther. 2023;29(7):438–447.