Bispecific Antibodies for the Treatment of Relapsed or Refractory Multiple Myeloma
Mikhaila Rice,1 PharmD, BCPS, BCOP, Beth Faiman,2 PhD, MSN, APN-BC, BMTCN, FAAN, FAPO, and Haleigh Mistry,3 MS, PA-C
From 1Department of Pharmacy, Cleveland Clinic, Cleveland, Ohio; 2Department of Hematologic Oncology and Blood Disorders, Taussig Cancer Institute, Cleveland, Ohio; 3Department of Lymphoma & Myeloma, MD Anderson Cancer Center, Houston, Texas.
Authors’ disclosures of conflicts of interest are found at the end of this article.
Correspondence to: Beth Faiman, PhD, MSN, APN-BC, BMTCN, FAAN, FAPO, Department of Hematologic Oncology and Blood Disorders, Taussig Cancer Institute, Cleveland, Ohio. E-mail: faimanb@ccf.org
Introduction
Multiple myeloma (MM) is the second most common hematologic malignancy in the United States, with an estimated 35,730 new cases and over 12,000 deaths in 2023 (Siegel et al., 2023). Many effective agents have been developed for the treatment of MM, including immunomodulatory drugs (IMiDs) such as thalidomide and lenalidomide, proteosome inhibitors (PIs) like bortezomib, and anti-CD38 monoclonal antibodies (mAbs), as well as high-dose therapy with autologous stem cell transplantation (ASCT). Second-generation agents such as pomalidomide, carfilzomib, and ixazomib have further improved outcomes, with some offering greater convenience of oral dosing. Additionally, two anti-CD38 mAbs, daratumumab and isatuximab, have been approved in combination with other agents for treatment of RRMM following ≥ 2 prior lines of therapy (LOT), and the anti-SLAM7 mAb elotuzumab was approved for RRMM in combination lenalidomide or pomalidomide (Figure 1; Brigle et al., 2022; Noonan et al., 2022). However, patients with MM inevitably relapse due to clonal heterogeneity and acquired resistance, while some are initially refractory. Those who are triple-class exposed have particularly poor outcomes, with an average overall response rate (ORR) of 31% and median overall survival (mOS) of approximately 9 months (Gandhi et al., 2019).
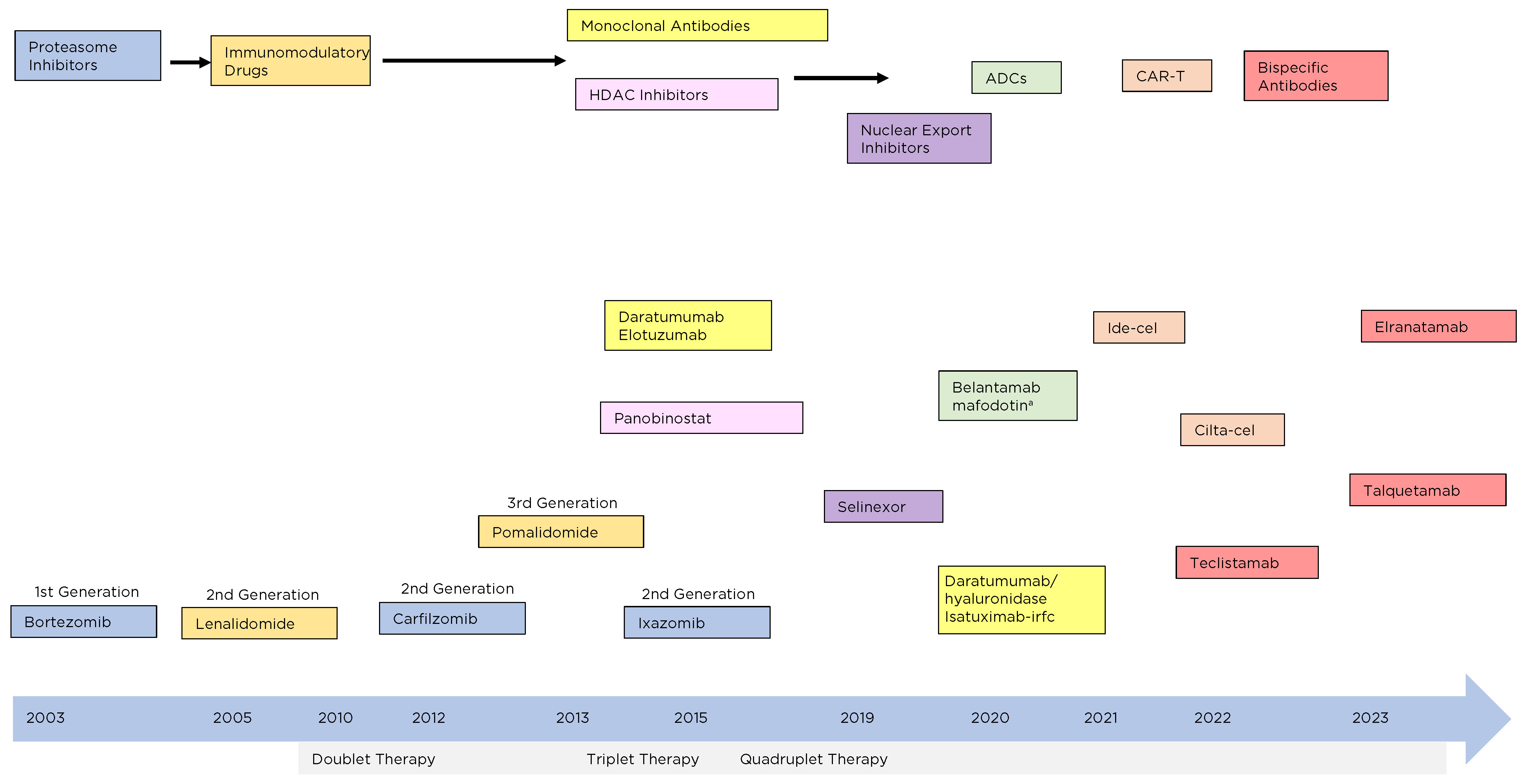
Figure 1. Timeline of development and approval of multiple myeloma therapeutics. ADCs = antibody-drug conjugates; CAR-T = chimeric antigen receptor T-cell therapy; cilta-cel = ciltacabtagene autoleucel; ide-cel = idecabtagene vicleucel. Adapted from Nishida (2021).
aBelantamab mafodotin withdrawn from US market in November 2022.
Currently, no standard of care exists for triple-class exposed patients. A prospective, multinational study (LocoMMotion) assessed real-life standard of care (SOC) in 248 triple-class exposed patients with relapsed or refractory disease (RRMM) who had received at least an IMiD, a PI, and an anti-CD38 mAb. More than 90 different treatment regimens were used, including IMiDs, PIs, mAbs, targeted agents, and alkylating agents. Not surprisingly, outcomes varied considerably, with an ORR of 29.8% (95% CI = 24.2–36.0), median progression-free survival (mPFS) of 4.6 months (95% CI = 3.9–5.6), and mOS of 12.4 months (95% CI = 10.3–not estimable; Mateos et al., 2022; Moreau et al., 2023). These data indicate the wide variability of regimens used in real-world settings and the generally poor outcomes for such patients. They also highlight the absence of a clear standard of care for heavily pretreated, triple-class exposed patients. Such results underscore the urgent need for more effective therapies relying on novel mechanisms of action for this patient population.
For patients with RRMM, current treatment guidelines indicate that choice of subsequent therapy depends in part on the number of prior therapies and whether the patient is still sensitive to bortezomib and/or lenalidomide. Numerous regimens are listed as preferred, with many others recommended. For patients with late relapses (> 3 prior therapies), treatment options are more limited. According to guidelines issued by the National Comprehensive Cancer Network (NCCN) and the International Myeloma Working Group, treatment options for patients with RRMM following > 3 prior therapies include bendamustine monotherapy, bendamustine-based combination regimens, and high-dose or fractionated cyclophosphamide (Table 1; NCCN, 2023; Moreau et al., 2021). Outcomes with bendamustine-based therapies tend to be better when such treatments are used earlier rather than later. A retrospective analysis found that PFS with bendamustine-based therapies was significantly greater in patients with 1 to 2 prior LOT compared with those who had received ≥ 3 LOT (10 months vs. 5 months; hazard ratio [HR] 0.472, 95% CI = 0.305–0.733; p < .001; Grzasko et al., 2021).

For RRMM patients who have received ≥ 4 prior therapies including an IMiD, a PI, and an anti-CD38 mAb, recommended treatment options are limited to only two chimeric antigen receptor T-cell therapies (CAR-T), idecabtagene vicleucel and ciltacabtagene autoleucel, and the bispecific antibodies (BsAb) teclistamab, talquetamab, and elranatamab; NCCN, 2023). (Belantamab mafodotin may be useful in certain cases if available through compassionate use program but has been withdrawn from the US market; see section on Antibody-Drug Conjugates.)
This review focuses on current treatment landscape and therapeutic options for heavily pretreated patients with RRMM following ≥ 4 prior LOT, particularly BsAbs, though CAR-T agents will be covered as well.
Bispecific Antibodies
Bispecific antibodies (BsAbs) are genetically engineered artificial antibodies that simultaneously target tumor antigens as well as CD3 expressed on the surface of T cells (Figure 2). BsAbs are designed to bind to MM cells that express a specific tumor antigen, such as B-cell maturation antigen (BCMA), CD38, or G protein-coupled receptor, class C, group 5, member D (GPRC5D), and also to effector T cells, generating a bridge between these cells and triggering an antitumor immune response (Cho et al., 2022). Such binding promotes T-cell activation, proliferation, and differentiation, and release of cytokines and growth factors, inducing an antitumor response and tumor cell lysis. In many cases, treatment with BsAbs results in fast and deep antitumor responses.
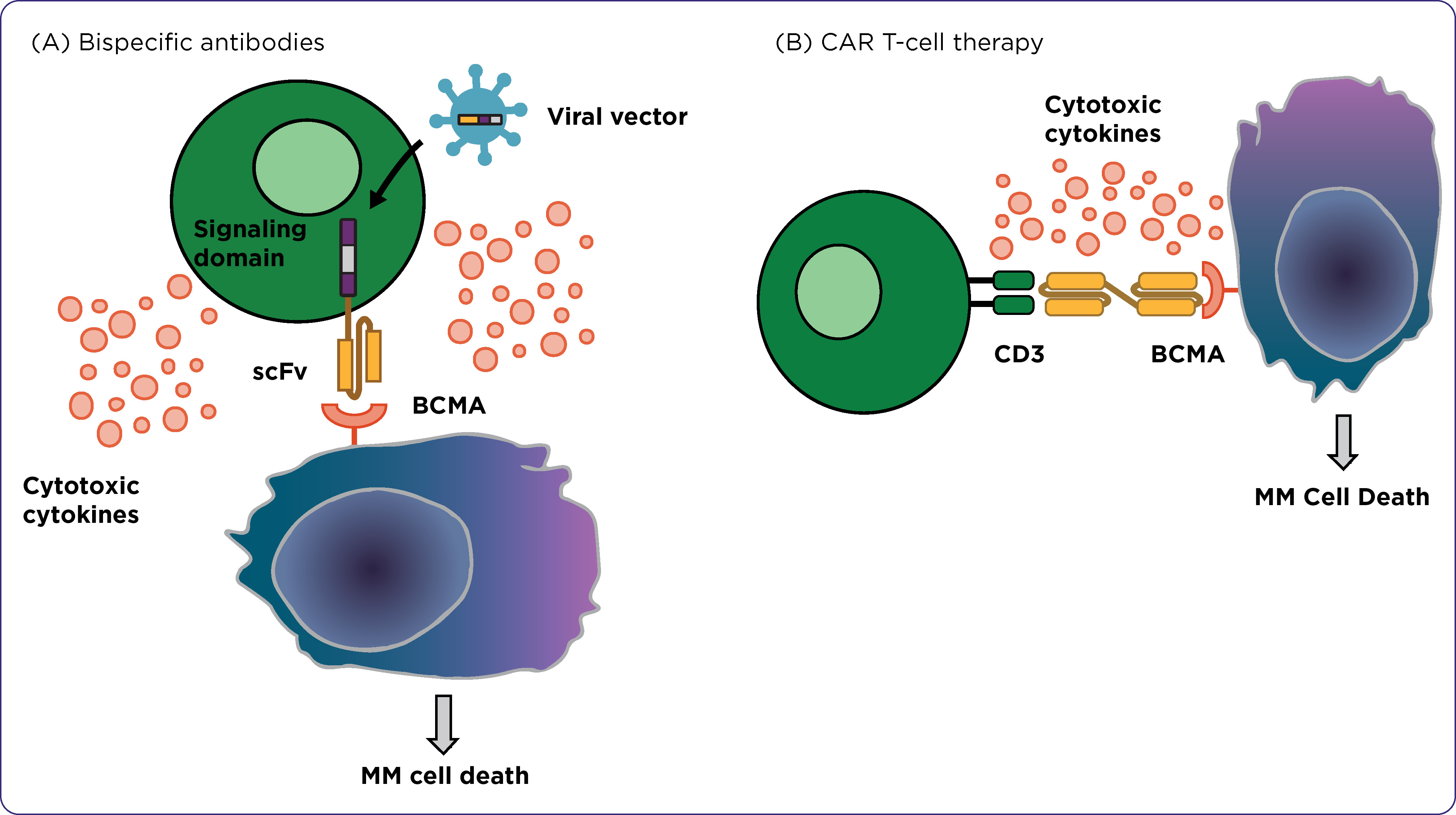
Figure 2. Mechanisms of action of BCMA-targeted bispecific antibodies and CAR T-cell therapy in multiple myeloma. scFv = single-chain variable fragment. Adapted from Yu et al. (2020).
Teclistamab
Teclistamab is a first-in-class, humanized, bispecific BsAb for treatment of RRMM. It was designed to bind to the CD3 receptor on T-cell surfaces and to BCMA on MM cells. BCMA (tumor necrosis factor receptor superfamily member 17) is a B-cell maturation antigen that is overexpressed on the surface of malignant plasma B cells and plays a role in MM pathogenesis, and therefore can serve as a rational therapeutic target (Wu et al., 2022). Binding of teclistamab to MM cells triggers release of proinflammatory cytokines and initiates destruction of target MM cells (Hua et al., 2022).
In vitro, teclistamab induced cytotoxicity of BCMA-positive MM cell lines and BCMA-positive cells in bone marrow samples from MM patients (Pillarisetti et al., 2020). In the first-in-human clinical trial (MajesTEC-1), teclistamab was administered to heavily pretreated MM patients who were triple-exposed (82% triple-refractory, 39% penta-refractory), including an IMiD, a PI, and anti-CD38 mAb. At a median follow-up of 14.1 months, a high rate of deep, durable responses was noted, with an ORR of 63% (95% CI = 55.2%–70.4%), including 39.4% with a complete response or better. For patients with a complete response (CR) or better, the minimal residual disease (MRD)-negativity rate was 46%. Median time to first response was 1.2 months and median duration of response (mDOR) was 18.4 months. With extended (22-month) follow-up, 43% of patients had a CR or better; mDOR was 24 months (not reached in patients with a CR), while mPFS and mOS were 12.5 months and 21.9 months, respectively (Moreau et al., 2022).
The efficacy observed with teclistamab in the MajesTEC-1 trial compares favorably to other available therapies for triple-class refractory RRMM. The relative effectiveness of teclistamab and real-world standard-of-care (SOC) therapies in triple-exposed patients was evaluated using individual patient data from the MajesTEC-1 and LocoMMotion trials. In adjusted comparisons, teclistamab was more likely to result in significantly better ORR, very good partial response (VGPR) or better, and complete response or better compared with SOC; DOR and PFS were also significantly increased (Moreau et al., 2023). Results of this analysis suggest that teclistamab therapy significantly improves response rate and survival compared with other SOC therapies in RRMM following ≥ 3 previous lines of therapy. Similar analyses suggest greater efficacy of teclistamab when results of the MajesTEC-1 trial were compared with studies using the antibody-drug conjugate belantamab mafodotin or the anti-CD38 mAb daratumumab in patients with triple-exposed RRMM (Moreau et al., 2022; Mateos et al., 2023). Teclistamab is now included in the NCCN Guidelines as a treatment option for patients with RRMM who have received ≥ 4 prior therapies, including an IMiD, a PI, and an anti-CD38 mAb (NCCN, 2023). Teclistamab might also have potential as an alternative to CAR-T for patients who cannot receive lymphodepleting chemotherapy (typically a combination of fludarabine and cyclophosphamide) ahead of CAR-T cell infusion or who are not candidates for CAR-T due to rapid progression of disease, poor organ function or performance status, lack of caregiver support, lymphopenia, or other patient-specific factors (Shah et al., 2020).
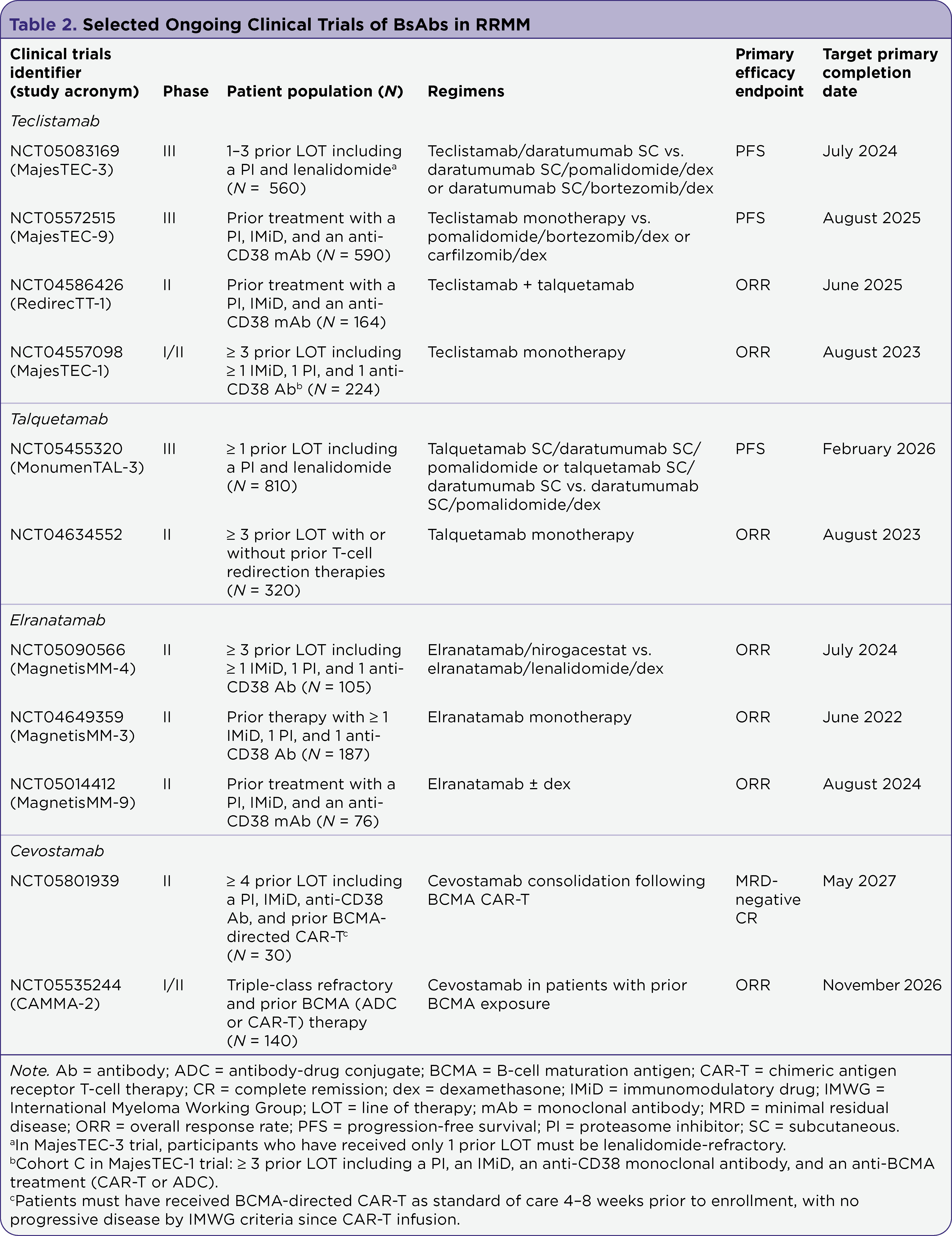
Several ongoing phase III trials are further evaluating teclistamab in heavily treated patients with RRMM (Table 2). The MajesTEC-3 phase III trial is comparing treatment with the combination of teclistamab and daratumumab to investigator’s choice of daratumumab, pomalidomide, and dexamethasone (DPd) or daratumumab, bortezomib, and dexamethasone (DVd) in patients with 1 to 3 prior LOT including a PI and lenalidomide. Another phase III trial, MajesTEC-9, will randomize patients with 1 to 3 prior LOT including a PI and lenalidomide to either teclistamab monotherapy or investigator's choice of pomalidomide, bortezomib, and dexamethasone (PVd) or carfilzomib and dexamethasone (Kd). Additionally, several trials are evaluating teclistamab for treatment of newly diagnosed MM, either alone or in combination with lenalidomide as maintenance therapy following ASCT (MajesTEC-4), in combination with daratumumab and lenalidomide (MajesTEC-7), or combined with daratumumab and talquetamab (GEM-TECTAL).
Elranatamab
Elranatamab (PF-3135) is a humanized BsAb targeting BCMA and CD3 that can also induce T-cell–mediated lysis of MM cells. Preliminary efficacy was seen in a phase I trial in patients with RRMM. Subsequently, the MagnestisMM-3 phase II trial evaluated elranatamab in this patient population following prior treatment with ≥ 1 IMiD, ≥ 1 PI, and ≥ 1 anti-CD38 mAb. In patients with no prior BCMA-directed therapy, at a median follow-up of 6.8 months, the ORR was 61%, with responses seen across subgroups. Time to objective response was rapid (1.2 months), and the mDoR had not yet been reached at time results were presented (Bahlis et al., 2022). At a follow-up of >1 year, the ORR was 61% (31.7% CR or stringent CR), and mPFS and mOS had not yet been reached (Mohty et al., 2023). A subsequent pooled analysis of MagnetisMM-3 and two other MagnetisMM trials of elranatamab in RRMM reported an ORR of 45.3%, with 17.4% CRs (Nooka et al., 2023). Data from the MagnestisMM-3 trial led to FDA accelerated approval in August 2023 of elranatamab for the treatment of adult patients with RRMM who have received ≥ 4 prior LOT including a PI, an IMiD, and an anti-CD38 mAb.
Ongoing phase II/III trials for patients with RRMM are comparing elranatamab monotherapy to elranatamab plus dexamethasone; single-agent elranatamab versus elranatamab plus lenalidomide or elranatamab plus nirogacestat (a γ-secretase inhibitor); and elranatamab monotherapy vs. elranatamab plus daratumumab or daratumumab plus pomalidomide.
Talquetamab
Talquetamab is a BsAb that binds to CD3 as well as GPRC5D, a receptor that is highly expressed on MM cells (Lakshman & Kumar, 2022). Talquetamab is the first and only currently approved therapy targeting the GPRC5D receptor. A phase I study (MonumenTAL-1) evaluated talquetamab monotherapy in patients RRMM who had received ≥ 3 prior LOT or were intolerant to or progressing on standard therapies. Triple-class–refractory disease was noted in 79% of patients, and 30% were penta-drug refractory. At a median follow-up of 11.7 months (405-mg dose level) and 4.2 months (800-mg dose level), responses were seen in 70% and 64% of patients, respectively, with a median DOR of 10.2 months and 7.8 months (Chari et al., 2022; Schinke et al., 2023). These results led to FDA accelerated approval of talquetamab in August 2023 for treatment of adult patients with RRMM who have previously received ≥ 4 prior LOT including a PI, an IMiD, and an anti-CD38 antibody (Janssen Pharmaceuticals, 2023a).
Talquetamab-based combination regimens may also have potential in this setting. The combination of talquetamab and daratumumab was evaluated in a phase I study (TRIMM-2) in patients with ≥ 3 prior LOT or who were double-refractory to a PI and an IMiD (with no prior anti-CD38 mAb). This regimen resulted in an ORR of 78% (66% ≥ very good partial responses, 45% ≥ CR), with responses largely durable for at least 1 year. The mPFS was 19.4 months (Dholaria et al., 2023). The ongoing RedirecTT-1 trial is exploring the combination of two BsAbs, talquetamab and teclistamab, in triple-exposed patients (78% triple-class refractory, 63% penta-drug exposed). At a median follow-up of 14.4 months, treatment at the recommended phase II dose resulted in an ORR of 92% (≥ CR 31%) among all evaluable patients and 83% (≥ CR 33%) in those with extramedullary disease (the mDOR had not been reached; Cohen et al., 2023). Safety data were consistent with the safety profiles of each individual agent. The data confirm the feasibility and safety of this dual BsAb combination designed to target distinct myeloma antigens. They also support the continued evaluation of this regimen for treatment of RRMM, particularly in patients with extramedullary disease who represent a high-risk population with an unmet need. The MonumenTAL-3 phase III trial is comparing regimens consisting of talquetamab and daratumumab, talquetamab, daratumumab, and pomalidomide, or daratumumab, pomalidomide, and dexamethasone in patients with RRMM who have received ≥ 1 prior LOT including a PI and lenalidomide.
Cevostamab
Cevostamab (BFCR4350A) is a humanized BsAb targeting CD3 and FcRH5 (Fc receptor-homolog 5), another antigen expressed on myeloma cells. Preclinical studies of cevostamab demonstrated its cytotoxicity against MM cells at low concentrations, and in monkeys cevostamab caused B-cell and bone marrow cell depletion. In vitro activity was enhanced when cevostamab was combined with an anti-PD-L1 antibody (Li et al., 2017). Updated results from a dose-escalation phase I trial in patients with triple-refractory RRMM reported a dose-dependent increase in ORR (54% at a dose of 160 mg). Responses were comparable in penta-drug refractory patients, and efficacy was seen in those with prior exposure to other BsAbs, CAR-Ts, antibody-drug conjugates, and anti-BCMA targeting agents (Trudel et al., 2021). Ongoing trials are further evaluating cevostamab in patients with prior BCMA-targeted therapy or CAR-T, and in combination with an IL-15Ra fusion protein (XmAb24306).
In addition to the above BsAbs, other BsAbs in development for RRMM include agents such as linvoseltamab, TNB-383B, alnuctamab, pavurutamab, RG2634, and GPRC5D TRAB. These are largely limited to early-phase clinical trials to date (Cho et al., 2022).
CAR T-Cell Therapy
CAR-T involves genetically altering a patient’s T cells to express an antigen-binding region that recognizes a specific tumor antigen and a T-cell binding epitope that activates and recruits cytotoxic T cells (Figure 2; Catamero et al., 2022). The 2017 approval of the CAR-T tisagenlecleucel for treatment of other selected B-cell malignancies led to clinical development of CAR-T products for RRMM. Newer constructs contain one or more costimulatory molecules such as CD28 or 4-1BB, in addition to the tumor antigen-binding antibody domain and CD3, that can further enhance antitumor responses. While most CAR T-cell therapy for MM targets BCMA, other B-cell antigens (e.g., CD19, SLAMF7, CD38) have also been evaluated. A meta-analysis of 23 trials, using various CAR-T constructs and target antigens, found this therapy to be efficacious in heavily pretreated RRMM patients. Furthermore, BCMA-directed therapies showed better efficacy than non–BCMA–targeted ones (Yang et al., 2023).
Currently, two CAR-T products are FDA approved for treatment of RRMM: idecabtagene vicleucel and ciltacabtagene autoleucel. Both are now included in NCCN guidelines as a treatment option for RRMM following ≥ 4 prior LOT including an IMiD, a PI, and an anti-CD38 mAb (NCCN, 2023). Idecabtagene vicleucel is a second-generation anti-BCMA CAR-T consisting of autologous T cells transduced with a lentiviral vector that expresses a chimeric antigen receptor (CAR) targeting BCMA; it also includes a transmembrane domain containing 4–1BB and CD3ζ chain T-cell intracellular signaling domains. The initial efficacy and tolerability of idecabtagene vicleucel was seen in a phase I trial in heavily pretreated patients who were refractory to an IMiD and a PI. In a subsequent phase II trial (KarMMa), an ORR of 81% (39% ≥ CR) and PFS of 12 months were reported. Activity was also seen in high-risk subgroups and patients with more advanced disease, and its efficacy was comparable in older and younger individuals. The mOS for all patients was 25 months (Munshi et al., 2021). These data led to FDA approval of idecabtagene vicleucel for patients with RRMM who have received ≥ 4 prior LOT including an IMiD, a PI, and an anti-CD38 mAb (Bristol Myers Squibb, 2021).
Ciltacabtagene autoleucel is the second anti-BCMA CAR-T product approved for treatment of RRMM. It is composed of two high-avidity, BCMA-targeting single-domain antibodies, a 4-1BB co-stimulatory domain, and a CD3ζ signaling cytoplasmic domain (Catamero et al., 2022). Its efficacy was established by the CARTITUDE-1 phase Ib/II trial in patients with RRMM following ≥ 3 prior LOT including an IMiD, a PI, and an anti-CD38 mAb. At the 2-year follow-up, the ORR was 97.9% (85% stringent CR); mPFS and mOS had not yet been reached (Berjeda et al., 2021; Martin et al., 2023). Results of the CARTITUDE-1 trial led to FDA approval of ciltacabtagene autoleucel for treatment of adult patients with RRMM after ≥ 4 prior LOT including an IMiD, a PI, and an anti-CD38 mAb (Janssen Pharmaceuticals, 2023b). Like idecabtagene vicleucel, ciltacabtagene autoleucel can induce early, deep, and long-lasting responses in this setting. In meta-analyses of indirect comparisons, ciltacabtagene autoleucel provides a significantly superior advantage compared to physicians’ treatment of choice, highlighting its effectiveness in patients with triple-class exposed RRMM (Costa et al., 2022).
The prescribing information for these two CAR-T products contains boxed warnings regarding risk of treatment-related cytokine release syndrome (CRS), immune effector-cell associated neurotoxicity syndrome (ICANS) and other neurologic toxicities, prolonged cytopenia, and hemophagocytic lymphohistiocytosis/macrophage activation syndrome (HLH/MAS), so clinicians should be aware of these risks and guidelines for prophylaxis and management (Murthy et al., 2022; Ludwig et al., 2023). Ciltacabtagene autoleucel also poses a risk of Guillain-Barré syndrome and parkinsonism.
Recent results suggest the potential for earlier use of CAR-T in the RRMM setting. In the KarMMa-3 phase III trial, for example, patients with RRMM who had previously received 2 to 4 regimens (including IMiDs, PIs, and daratumumab) and whose disease was refractory to the last line of therapy were randomized to treatment with idecabtagene vicleucel or standard MM regimens. At a median follow-up of 18.6 months, mPFS was significantly improved with idecabtagene vicleucel compared to SOC (13.3 months vs. 4.4 months; (HR 0.49; p < .0001) and was seen across all patient subgroups. OS data are not yet mature. The safety profile was similar that the toxicity of idecabtagene vicleucel in later RRMM settings (Rodriguez-Otero et al., 2023).
Antibody-Drug Conjugates
Antibody-drug conjugates (ADCs) represent another approach being evaluated for heavily pretreated RRMM. These agents consist of a tumor-specific mAb coupled to a highly active cytotoxin via a cleavable or noncleavable linker. ADCs are designed to deliver high local concentrations of cytotoxin to tumor cells, resulting in apoptosis. Many ADCs have proved effective for treatment of selected solid tumors and lymphomas, and to date at least 12 agents have been FDA approved for various indications (Esapa et al., 2023). Multiple ADCs are currently in clinical trials for RRMM, targeting BCMA, CD38, FcRH5, or other tumor antigens and using various cytotoxic payloads (Ray & Orlowski, 2023).
Belantamab mafodotin is a first-in-class ADC composed of an anti-BCMA antibody linked to the microtubule inhibitor monomethyl aurostatin F. The phase II DREAMM-2 trial evaluated belantamab mafodotin in RRMM patients following ≥ 3 prior LOT who were refractory to IMiDs and PIs, and refractory or intolerant (or both) to an anti-CD38 mAb. Responses were seen in 34% of patients at the 3.4-mg dose level (Lonial et al., 2020). These results led to FDA approval of this ADC in 2020 for treatment of RRMM following ≥ 4 prior therapies including an IMiD, a PI, and an anti-CD38 mAb. However, a confirmatory phase III trial (DREAMM-3) found no significant improvement in PFS with belantamab mafodotin compared to pomalidomide plus dexamethasone, resulting in withdrawal of this ADC from the US market (Weisel et al., 2023). This agent is now available only for patients who began such treatment prior to its withdrawal from market and are continuing to respond to and tolerate therapy. Ongoing studies are evaluating belantamab mafodotin in combination with other agents to further enhance efficacy in RRMM.
Selection of BsAb vs CAR-T for RRMM
Treatment decisions regarding selection of BsAbs, CAR-T, or other therapies for heavily treated patients with RRMM requires consideration of multiple factors. When choosing therapy, clinicians should consider patient age, performance status, comorbidities, prior therapies and response, patient preference, and possible effects on quality of life in addition to expected efficacy and treatment-related toxicity (Dimopoulos et al., 2022).
While both BsAbs and CAR-T are effective for RRMM, the former offer a number of potential advantages. BsAbs are more widely available, allowing use of “off-the-shelf” products rather than waiting for production of a patient-customized CAR-T product and thus avoiding delays in treatment initiation. BsAbs are less complicated to administer, may result in less target antigen loss, and can often achieve similar efficacy as CAR-T (although response rates with BsAbs may be lower, especially compared to ciltacabtagene autoleucel). BsAbs are associated with a lower risk of severe immune-related adverse events such as CRS and ICANs compared with CAR-T. Upfront costs of BsAbs are relatively low compared to CAR-T; however, unlike CAR-T, patients receiving BsAbs require ongoing treatment, and total treatment-related costs will increase with time on therapy. CAR-T and BsAbs therapies are currently only available at select institutions, so indirect costs such as travel and lodging for patients and their caregivers must also be considered (Ghanem & Shi, 2022).
Potential advantages of CAR-T include high response rates, durable responses, and the possible need for only a single infusion compared with longer-term BsAb therapy. CAR-T may be more convenient for some patients: although close monitoring or hospitalization is necessary for CAR T-cell infusion, subsequent follow-up requirements are limited. In contrast, BsAb therapy requires patients to return to treatment centers for weekly injections (or every other week for talquetamab). Limitations of CAR-T include the need to customize treatment for each patient, impaired in vivo persistence, potential for resistance/relapse, production complexity, lengthy development time (≥ 4 weeks) that may necessitate use of bridging therapy, limited production capacity, and manufacturer restrictions on allotted number of treatments per facility. CAR-T also requires patients to have adequate performance status to undergo lymphodepletion, and to remain stable throughout the collection and processing procedures. Efforts are ongoing to develop “off-the-shelf” universal CAR-T products that could broaden its use for RRMM and other B-cell malignancies, reduce costs, and shorten manufacturing delays.
Sequencing
Questions remain regarding the optimal sequencing of BsAbs and CAR-T, particularly for patients previously treated with anti-BCMA agents or who are resistant to one of these classes of therapies. A literature review found that in RRMM patients previously treated with BCMA-directed therapy, BsAbs and CAR-T can both generate clinically meaningful benefit and durable response rates. The highest ORRs were seen with idecabtagene vicleucel (74%) and the combination of talquetamab and daratumumab (72%), although all agents were effective (Patel et al., 2023). A recent study evaluated ciltacabtagene autoleucel treatment in 20 heavily pretreated patients with RRMM and disease progression after prior anti-BCMA therapy. At a median follow-up of 11.3 months, the ORR was 60%, with a mDOR of 11.5 months and mPFS of 9.1 months (Cohen et al., 2023). These data suggest that patients previously treated with BCMA-targeted therapy may yet respond to ciltacabtagene autoleucel upon progression. Whether this also applies to ide-cel, or to patients who previously received non-BCMA BsAbs or CAR-T, remains to be determined. The optimal sequencing strategy using BsAbs and CAR-T remains to be determined.
Some studies suggest the feasibility of sequential BsAb and CAR-T therapy to target the same or distinct myeloma antigens. Preliminary data from a cohort of patients in the MajesTEC-1 trial who had prior exposure to other anti-BCMA therapy indicates they might still respond to the anti-BCMA BsAb teclistamab. In this study, triple-exposed patients with RRMM who were previously treated with ≥ 3 prior LOT including an IMiD, a PI, an anti-CD38 antibody, and anti-BCMA CAR-T or anti-BCMA ADC (median of 6 prior LOT) received weekly teclistamab. Among 25 efficacy-evaluable patients, the ORR was 40% (95% CI = 21–61), with a CR or better in 20% of patients; mDOR was not reached (Touzeau et al., 2022). These preliminary results suggest that serial targeting of BCMA with teclistamab following prior BCMA-directed therapy could be an effective approach for some patients. A few small studies have also evaluated sequential therapy using CAR-T products directed against different target antigens in an effort to improve responses. A pilot study of 10 patients with RRMM treated sequentially with CD19-CAR-T and BCMA-CAR-T demonstrated the feasibility of this approach, although the 3 patients who received allogeneic CAR-T experienced rapid disease progression compared with those who received autologous infusions (Yan et al., 2021).
Resistance to BsAbs and CAR-T can develop in patients with RRMM. Mechanisms of resistance to these therapies are not fully understood, and no method of testing for resistance currently exists. Resistance may be suggested by observed disease response, such as in patients with prior BsAbs or CAR-T exposure who fail to achieve an adequate response with initiation of a new BsAb or CAR-T product, or in patients who progress on current BsAb or CAR-T therapy. With BsAbs, continuous antigen exposure and an inhibitory tumor microenvironment may lead to T-cell exhaustion, resulting in development of resistance (Swan et al., 2023). Similarly, loss of BCMA target antigen and expansion of BCMA-negative MM cells could lead to decreased CAR-T response. Regimens combining BsAbs with cytotoxic agents or other immunotherapeutics might help overcome the MM immunosuppressive microenvironment and prevent or delay development of resistance. Targeting non-BCMA tumor antigens may also obviate resistance to BCMA-directed therapy. Additionally, novel CAR-T products that simultaneously target different tumor antigens are being investigated, which might prevent development of resistance occurring due to loss of target antigen (Lakshman & Kumar, 2022). Next-generation CAR-T that secrete inflammatory cytokines or anti-immune checkpoint inhibitor antibodies could overcome resistance and further enhance antimyeloma responses (Sammartano et al., 2023).
Conclusion
Immunotherapy has revolutionized the treatment of MM, with the availability of numerous active agents. However, many are not effective for patients with late relapses. For heavily pretreated RRMM patients who are triple-refractory and require further therapy, BsAbs and CAR-T offer novel treatment options that can result in clinically meaningful responses for this difficult-to-treat patient population.
To date three BsAbs—teclistamab, talquetamab, and elranatamab—have been approved for treatment of RRMM after ≥ 4 prior LOT. In addition to the recently approved talquetamab and elranatamab, other BsAbs could receive regulatory approval for this indication in the near future. Further research is needed to determine the efficacy of these agents in patients exposed to other BCMA-directed treatments, the benefits of dual BsAb therapy (e.g., teclistamab combined with talquetamab), and the potential of BsAbs combined with other classes of MM therapy.
BsAbs may also be good treatment option for patients who have progressed following CAR-T, in patients who are ineligible for CAR-T, and those who are unable to wait for CAR-T collection and production due to disease progression. Results of ongoing clinical trials could demonstrate the potential of BsAbs in earlier lines of treatment. These efforts may further improve outcomes and quality of life for an even wider patient population that previously had few therapeutic options.
Acknowledgment
Writing assistance was provided by Larry Rosenberg, PhD.
Disclosure
Dr. Faiman has served as a consultant for Amgen, BMS, Janssen, and Pfizer. Dr. Rice has served on the advisory board for Janssen. Ms. Mistry has no conflict of interest to disclose.
References
Bahlis, N. J., Tomasson, M. H., Mohty, M., Niesvizky, R., Nooka, A. K., Manier, S.,...Lesokhin, A. M. (2022). Efficacy and safety of elranatamab in patients with relapsed/refractory multiple myeloma naive to B-cell maturation antigen (BCMA)-directed therapies: Results from cohort a of the Magnetismm-3 study. Blood, 140(Suppl 1), 391–393. https://doi.org/10.1182/blood-2022-162440
Berdeja, J. G., Madduri, D., Usmani, S. Z., Jakubowiak, A., Agha, M., Cohen, A. D.,… Jagannath, S. (2021). Ciltacabtagene autoleucel, a B-cell maturation antigen-directed chimeric antigen receptor T-cell therapy in patients with relapsed or refractory multiple myeloma (CARTITUDE-1): A phase 1b/2 open-label study. Lancet (London, England), 398(10297), 314–324. https://doi.org/10.1016/S0140-6736(21)00933-8
Brigle, K., Verina, D., & Faiman, B. (2022). A focus on newly diagnosed multiple myeloma. Journal of the Advanced Practitioner in Oncology, 13(suppl 4), 7–14. https://doi.org/10.6004/jadpro.2022.13.5.10
Bristol Myers Squibb. (2021). Abecma (idecabtagene vicleucel) package insert. https://packageinserts.bms.com/pi/pi_abecma.pdf
Catamero, D., Richards, T., & Faiman, B. (2022). A focus on CAR T-cell therapy and bispecific antibodies in multiple myeloma. Journal of the Advanced Practitioner in Oncology, 13(suppl 4), 31–43. https://doi.org/10.6004/jadpro.2022.13.5.13
Chari, A., Touzeau, C., Schinke, C., Minnema, M. C., Berdeja, J., Oriol, A.,…Moreau, P. (2022). Talquetamab, a G protein-coupled receptor family C group 5 member D x CD3 bispecific antibody, in patients with relapsed/refractory multiple myeloma (RRMM): Phase 1/2 results from MonumenTAL-1. Blood, 140(suppl 1), 384–387.
Cho, S. F., Yeh, T. J., Anderson, K. C., & Tai, Y. T. (2022). Bispecific antibodies in multiple myeloma treatment: A journey in progress. Frontiers in Oncology, 12, 1032775. https://doi.org/10.3389/fonc.2022.1032775
Cohen, A. D., Mateos, M. V., Cohen, Y. C., Rodriguez-Otero, P., Paiva, B., van de Donk, N. W. C. J.,…San-Miguel, J. (2023). Efficacy and safety of cilta-cel in patients with progressive multiple myeloma after exposure to other BCMA-targeting agents. Blood, 141(3), 219–230. https://doi.org/10.1182/blood.2022015526
Cohen, Y. C., Morillo, D., Gatt, M. E., Sebag, M., Kim, K., Min, C.-K.,…Magen, H. (2023). First results from the RedirecTT-1 study with teclistamab (tec) + talquetamab (tal) simultaneously targeting BCMA and GPRC5D in patients (pts) with relapsed/refractory multiple myeloma (RRMM). Journal of Clinical Oncology, 41(16 suppl), 8002. https://doi.org/10.1200/JCO.2023.41.16_suppl.8002
Costa, L. J., Hari, P., Berdeja, J. G., De Stefano, V., Gay, F., Hooper, B.,…Weisel, K. (2022). Meta-analysis of ciltacabtagene autoleucel versus physician’s choice therapy for the treatment of patients with relapsed or refractory multiple myeloma. Current Medical Research and Opinion, 38(10), 1759–1767. https://doi.org/10.1080/03007995.2022.2100651
Dholaria, B. R., Weisel, K., Mateos, M.-V., Goldschmidt, H., Martin, T. G., Morillo, D.,…Chari, A. (2023). Talquetamab (tal) + daratumumab (dara) in patients (pts) with relapsed/refractory multiple myeloma (RRMM): Updated TRIMM-2 results. Journal of Clinical Oncology, 41(16 suppl), 8003. https://doi.org/10.1200/JCO.2023.41.16_suppl.8003
Dimopoulos, M. A., Richardson, P., & Lonial, S. (2022). Treatment options for patients with heavily pretreated relapsed and refractory multiple myeloma. Clinical Lymphoma, Myeloma & Leukemia, 22(7), 460–473. https://doi.org/10.1016/j.clml.2022.01.011
Esapa, B., Jiang, J., Cheung, A., Chenoweth, A., Thurston, D. E., & Karagiannis, S. N. (2023). Target antigen attributes and their contributions to clinically approved antibody-drug conjugates (ADCs) in haematopoietic and solid cancers. Cancers, 15(6), 1845. https://doi.org/10.3390/cancers15061845
Formulary Watch. (2022). Updated: FDA approves first bispecific antibody for multiple myeloma. https://www.formularywatch.com/view/fda-approves-first-bispecific-antibody-for-multiple-myeloma
Gandhi, U. H., Cornell, R. F., Lakshman, A., Gahvari, Z. J., McGehee, E., Jagosky, M. H.,…Costa, L. J. (2019). Outcomes of patients with multiple myeloma refractory to CD38-targeted monoclonal antibody therapy. Leukemia, 33(9), 2266–2275. https://doi.org/10.1038/s41375-019-0435-7
Ghanem, B., & Shi, L. (2022). The economic burden of CAR T cell therapies ciltacabtagene autoleucel and idecabtagene vicleucel for the treatment of adult patients with relapsed or refractory multiple myeloma in the US. BioDrugs, 36(6), 773–780. https://doi.org/10.1007/s40259-022-00557-3
Grzasko, N., Charlinski, G., Morawska, M., Kicinski, P., Waszczuk-Gajda, A., Drozd-Sokolowska, J.,…Giannopoulos, K. (2021). Bendamustine-based regimens as salvage therapy in refractory/relapsed multiple myeloma patients: A retrospective real-life analysis by the Polish Myeloma Group. Journal of Clinical Medicine, 10(23), 5504. https://doi.org/10.3390/jcm10235504
Hua, G., Scanlan, R., Straining, R., & Carlson, D. S. (2023). Teclistamab-cqyv: The first bispecific T-cell engager antibody for the treatment of patients with relapsed or refractory multiple myeloma. Journal of the Advanced Practitioner in Oncology, 14(2), 163–171. https://doi.org/10.6004/jadpro.2023.14.2.7
Janssen Pharmaceuticals. (2023a). Talvey (talquetamab-tgvs) package insert. https://www.janssenlabels.com/package-insert/product-monograph/prescribing-information/TALVEY-pi.pdf
Janssen Pharmaceuticals. (2023b). Carvykti (ciltacabtagene autoleucel) package insert. https://www.janssenlabels.com/package-insert/product-monograph/prescribing-information/CARVYKTI-pi.pdf
Lakshman, A., & Kumar, S. K. (2022). Chimeric antigen receptor T-cells, bispecific antibodies, and antibody-drug conjugates for multiple myeloma: An update. American Journal of Hematology, 97(1), 99–118. https://doi.org/10.1002/ajh.26379
Li, J., Stagg, N. J., Johnston, J., Harris, M. J., Menzies, S. A., DiCara, D.,…Junttila, T. T. (2017). Membrane-proximal epitope facilitates efficient T cell synapse formation by anti-FcRH5/CD3 and Is a requirement for myeloma cell killing. Cancer Cell, 31(3), 383–395. https://doi.org/10.1016/j.ccell.2017.02.001
Lonial, S., Lee, H. C., Badros, A., Trudel, S., Nooka, A. K., Chari, A.,… Cohen, A. D. (2020). Belantamab mafodotin for relapsed or refractory multiple myeloma (DREAMM-2): A two-arm, randomised, open-label, phase 2 study. Lancet Oncology, 21(2), 207–221. https://doi.org/10.1016/S1470-2045(19)30788-0
Ludwig, H., Terpos, E., van de Donk, N., Mateos, M. V., Moreau, P., Dimopoulos, M. A.,…Sonneveld, P. (2023). Prevention and management of adverse events during treatment with bispecific antibodies and CAR T cells in multiple myeloma: A consensus report of the European Myeloma Network. Lancet Oncology, 24(6), e255–e269. https://doi.org/10.1016/S1470-2045(23)00159-6
Martin, T., Usmani, S. Z., Berdeja, J. G., Agha, M., Cohen, A. D., Hari, P.,… Jagannath, S. (2023). Ciltacabtagene autoleucel, an anti-B-cell maturation antigen chimeric antigen receptor T-cell therapy, for relapsed/refractory multiple myeloma: CARTITUDE-1 2-year follow-up. Journal of Clinical Oncology, 41(6), 1265–1274. https://doi.org/10.1200/JCO.22.00842
Mateos, M. V., Chari, A., Usmani, S. Z., Goldschmidt, H., Weisel, K., Qi, K.,…Moreau, P. (2023). Comparative efficacy of teclistamab versus physician’s choice of therapy in the long-term follow-up of APOLLO, POLLUX, CASTOR, and EQUULEUS clinical trials in patients with triple-class exposed relapsed or refractory multiple myeloma. Clinical Lymphoma, Myeloma & Leukemia, 23(5), 385–393. https://doi.org/10.1016/j.clml.2023.02.006
Mateos, M. V., Weisel, K., De Stefano, V., Goldschmidt, H., Delforge, M., Mohty, M.,…Moreau, P. (2022). LocoMMotion: A prospective, non-interventional, multinational study of real-life current standards of care in patients with relapsed and/or refractory multiple myeloma. Leukemia, 36(5), 1371–1376. https://doi.org/10.1038/s41375-022-01531-2
Mohty, M., Tomasson, M. H., Arnulf, B., Bahlis, N. J., Prince, H. M., Niesvizky, R.,…Lesokhin, A. M. (2023). Elranatamab, a B-cell maturation antigen (BCMA)-CD3 bispecific antibody, for patients (pts) with relapsed/refractory multiple myeloma (RRMM): Extended follow up and biweekly administration from the MagnetisMM-3 study. Journal of Clinical Oncology, 41(16 suppl), 8039. https://doi.org/10.1200/JCO.2023.41.16_suppl.8039
Moreau, P., Garfall, A. L., van de Donk, N. W. C. J., Nahi, H., San-Miguel, J. F., Oriol, A.,…Usmani, S. Z. (2022). Teclistamab in relapsed or refractory multiple myeloma. New England Journal of Medicine, 387(6), 495–505. https://doi.org/10.1056/NEJMoa2203478
Moreau, P., Kumar, S. K., San Miguel, J., Davies, F., Zamagni, E., Bahlis, N.,…Richardson, P. G. (2021). Treatment of relapsed and refractory multiple myeloma: recommendations from the International Myeloma Working Group. Lancet Oncology, 22(3), e105–e118. https://doi.org/10.1016/S1470-2045(20)30756-7
Moreau, P., Usmani, S. Z., van de Donk, N. W. C. J., Garfall, A. L., Delforge, M., Rocafiguera, A. O.,…Krishnan, A. Y. (2022). Matching-adjusted indirect treatment comparison (MAIC) of teclistamab (tec) versus belantamab mafodotin (belamaf) for the treatment of patients (pts) with triple-class exposed (TCE), relapsed/refractory multiple myeloma (RRMM). Journal of Clinical Oncology, 40(16 suppl), 8035. https://doi.org/10.1200/JCO.2022.40.16_suppl.8035
Moreau, P., van de Donk, N. W. C. J., Delforge, M., Einsele, H., De Stefano, V., Perrot, A.,…Mateos, M. V. (2023). Comparative efficacy of teclistamab versus current treatments in real-world clinical practice in the prospective LocoMMotion study in patients with triple-class-exposed relapsed and/or refractory multiple myeloma. Advances in Therapy, 40(5), 2412–2425. https://doi.org/10.1007/s12325-023-02480-7
Munshi, N. C., Anderson, L. D., Jr, Shah, N., Madduri, D., Berdeja, J., Lonial, S.,…San-Miguel, J. (2021). Idecabtagene vicleucel in relapsed and refractory multiple myeloma. New England Journal of Medicine, 384(8), 705–716. https://doi.org/10.1056/NEJMoa2024850
Murthy, H. S., Yassine, F., Iqbal, M., Alotaibi, S., Moustafa, M. A., & Kharfan-Dabaja, M. A. (2022). Management of CAR T-cell related toxicities: What did the learning curve teach us so far? Hematology/Oncology and Stem Cell Therapy, 15(3), 100–111. https://doi.org/10.56875/2589-0646.1029
National Comprehensive Cancer Network. (2023). NCCN Clinical Practice Guidelines in Oncology: Multiple Myeloma. https://www.nccn.org/professionals/physician_gls/pdf/myeloma.pdf
Nishida, H. (2021). Rapid progress in immunotherapies for multiple myeloma: An updated comprehensive review. Cancers (Basel), 13(11), 2712. https://doi.org/10.3390/cancers13112712
Nooka, A. K., Lesokhin, A. M., Mohty, M., Niesvizky, R., Maisel, C., Arnulf, B.,…Yanovsky, A. V. (2023). Efficacy and safety of elranatamab in patients with relapsed/refractory multiple myeloma (RRMM) and prior B-cell maturation antigen (BCMA)-directed therapies: A pooled analysis from MagnetisMM studies. Journal of Clinical Oncology, 41(16 suppl), 8008. https://doi.org/10.1200/JCO.2023.41.16_suppl.8008
Noonan, K., Rome, S., & Faiman, B. (2022). A focus on relapsed multiple myeloma. Journal of the Advanced Practitioner in Oncology, 13(suppl 4), 15–21. https://doi.org/10.6004/jadpro.2022.13.5.11
Patel, U., Oluwole, O. O., Kassim, A., Jayani, R., Belliveau, P., Savani, B.,…Dholaria, B. R. (2023). Sequencing bispecific antibodies and CAR T cell therapy in multiple myeloma with prior exposure to BCMA-targeted therapies. Journal of Clinical Oncology, 41(16 suppl), 20049. https://doi.org/10.1200/JCO.2023.41.16_suppl.e20049
Pfizer. (2023). Elrexfio (elranatamab-bcmm) package insert. https://labeling.pfizer.com/ShowLabeling.aspx?id=19669
Pillarisetti, K., Powers, G., Luistro, L., Babich, A., Baldwin, E., Li, Y.,…Attar, R. (2020). Teclistamab is an active T cell-redirecting bispecific antibody against B-cell maturation antigen for multiple myeloma. Blood Advances, 4(18), 4538–4549. https://doi.org/10.1182/bloodadvances.2020002393
Ray, U., & Orlowski, R. Z. (2023). Antibody-drug conjugates for multiple myeloma: Just the beginning, or the beginning of the end? Pharmaceuticals (Basel, Switzerland), 16(4), 590. https://doi.org/10.3390/ph16040590
Rodriguez-Otero, P., Ailawadhi, S., Arnulf, B., Patel, K., Cavo, M., Nooka, A. K.,…Giralt, S. (2023). Ide-cel or standard regimens in relapsed and refractory multiple myeloma. New England Journal of Medicine, 388(11), 1002–1014. https://doi.org/10.1056/NEJMoa2213614
Sammartano, V., Franceschini, M., Fredducci, S., Caroni, F., Ciofini, S., Pacelli, P.,…Gozzetti, A. (2023). Anti-BCMA novel therapies for multiple myeloma. Cancer Drug Resistance, 6(1), 169–181. https://doi.org/10.20517/cdr.2022.138
Schinke, C. D., Touzeau, C., Minnema, M. C., van de Donk, N. W., Rodríguez-Otero, P., Mateos, M.-V.,…Chari, A. (2023). Pivotal phase 2 MonumenTAL-1 results of talquetamab (tal), a GPRC5DxCD3 bispecific antibody (BsAb), for relapsed/refractory multiple myeloma (RRMM). Journal of Clinical Oncology, 41(16 suppl), 8036. https://doi.org/10.1200/JCO.2023.41.16_suppl.8036
Shah, N., Chari, A., Scott, E., Mezzi, K., & Usmani, S. Z. (2020). B-cell maturation antigen (BCMA) in multiple myeloma: Rationale for targeting and current therapeutic approaches. Leukemia, 34(4), 985–1005. https://doi.org/10.1038/s41375-020-0734-z
Siegel, R. L., Miller, K. D., Wagle, N. S., & Jemal, A. (2023). Cancer statistics, 2023. CA: A Cancer Journal for Clinicians, 73(1), 17–48. https://doi.org/10.3322/caac.21763
Swan, D., Murphy, P., Glavey, S., & Quinn, J. (2023). Bispecific antibodies in multiple myeloma: opportunities to enhance efficacy and improve safety. Cancers (Basel), 15(6), 1819. https://doi.org/10.3390/cancers15061819
Touzeau, C., Krishnan, A., Moreau, P., Perrot, A., Usmani, S. Z., Manier, S.,…Garfall A. (2022). Evaluating teclistamab in patients with relapsed/refractory multiple myeloma following exposure to other B-cell maturation antigen (BCMA)-targeted agents. HemaSphere, 6, 85–86. https://doi.org/10.1097/01.HS9.0000843628.63947.e4
Trudel, S., Cohen, A., Krishnan, A., Fonseca, R., Spencer, A., Berdeja, J. G.,...Harrison, S. J. (2021). Cevostamab monotherapy continues to show clinically meaningful activity and manageable safety in patients with heavily pre-treated relapsed/refractory multiple myeloma (RRMM): Updated results from an ongoing phase I study. Blood, 138(suppl 1), 157.
Weisel, K., Hungria, V. T. M., Radinoff, A., Delimpasi, S., Mikala, G., Masszi, T.,…Dimopoulos, M. A. (2023). A phase 3, open-label, randomized study to evaluate the efficacy and safety of single-agent belantamab mafodotin (belamaf) compared to pomalidomide plus low-dose dexamethasone (Pd) in patients (pts) with relapsed/refractory multiple myeloma (RRMM): DREAMM-3. Journal of Clinical Oncology, 41(suppl 16), 8007. https://doi.org/10.1200/JCO.2023.41.16_suppl.8007
Wu, L., Huang, Y., Sienkiewicz, J., Sun, J., Guiang, L., Li, F.,…Golubovskaya, V. (2022). Bispecific BCMA-CD3 antibodies block multiple myeloma tumor growth. Cancers, 14(10), 2518. https://doi.org/10.3390/cancers14102518
Yan, L., Qu, S., Shang, J., Shi, X., Kang, L., Xu, N.,…Fu, C. (2021). Sequential CD19 and BCMA-specific CAR T-cell treatment elicits sustained remission of relapsed and/or refractory myeloma. Cancer Medicine, 10(2), 563–574. https://doi.org/10.1002/cam4.3624
Yang, Q., Li, X., Zhang, F., Yang, Q., Zhou, W., & Liu, J. (2021). Efficacy and safety of CAR-T therapy for relapse or refractory multiple myeloma: A systematic review and meta-analysis. International Journal of Medical Sciences, 18(8), 1786–1797. https://doi.org/10.7150/ijms.46811
Yu, B., Jiang, T., & Liu, D. (2020). BCMA-targeted immunotherapy for multiple myeloma. Journal of Hematology & Oncology, 13(1). https://doi.org/10.1186/s13045-020-00962-7
Zhang, X., Zhang, H., Lan, H., Wu, J., & Xiao, Y. (2023). CAR-T cell therapy in multiple myeloma: Current limitations and potential strategies. Frontiers in Immunology, 14, 1101495. https://doi.org/10.3389/fimmu.2023.1101495