Young Female With Thrombocytosis and Cerebrovascular Accident Post-COVID
Presentation
Ms. B is a 45-year-old healthy female with history of anxiety, migraine with aura, and recent COVID infection who presented to the emergency department (ED) with complaints of right-hand numbness and tingling and impaired speech. Regarding her prior COVID infection, she stated that symptoms started two weeks prior to the ED visit, were limited to the upper respiratory tract, and had resolved within one week.
ED Workup and Diagnosis
Ms. B underwent the following urgent imaging studies while in the ED:
- Head/neck CT angiography: Intraluminal thrombus extending into the proximal left external carotid artery and internal carotid artery (ICA) with short segment critical stenosis of the ICA
- Brain MRI: Moderate acute left middle cerebral artery gray and white matter infarcts
- Echocardiogram: Unremarkable left atrium, ejection fraction 60%-65%
Complete blood count (CBC) in the ED revealed thrombocytosis with a platelet count of 795 x 10⁹/L. This was thought to be possibly reactive in the setting of recent COVID infection; however, Ms. B mentioned that her platelets have been elevated for the past year for unknown reason.
Ms. B was diagnosed with a subacute left frontal periventricular ischemic stroke in the setting of left ICA thrombus and admitted to the neurological ICU for management and close monitoring. Her symptoms resolved with the initiation of anticoagulation, and no thrombectomy was needed. She was discharged on apixaban 5 mg BID. She was referred to hematology given the need for hypercoagulable workup and investigation of thrombocytosis.
Hematology Workup and Diagnosis
Ms. B had a repeat CBC in the hematology office at consultation, which revealed the following:
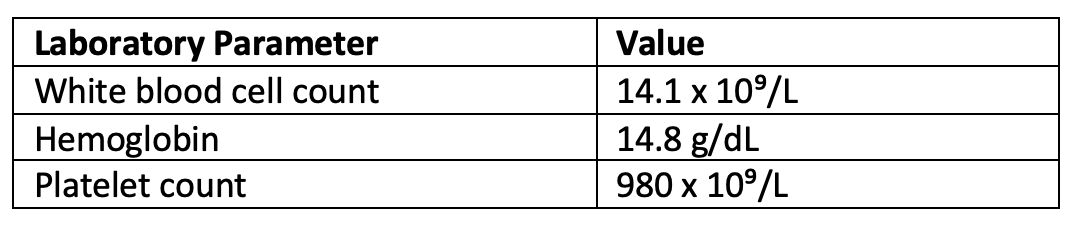
Standard hypercoagulable workup was negative, and iron levels were adequate. An MPN profile (JAK2, MPL, and CALR) to evaluate for the presence of molecular mutations was assessed on the peripheral blood, which resulted in the identification of CALR type 1 mutation. Based on the presentation, Ms. B was diagnosed with presumed essential thrombocytosis. A bone marrow aspiration and biopsy was discussed to rule out prefibrotic myelofibrosis; however, this was pursued at a later date due to safety concerns about holding anticoagulation in the acute post-stroke setting.
Treatment
For Ms. B, with a new diagnosis of a CALR+ MPN and thrombotic event, cytoreductive therapy and thrombosis prophylaxis are recommended. Several available therapies including hydroxyurea, interferons, and anagrelide were discussed, and she opted to pursue hydroxyurea. She tolerated this well with a quick reduction in platelet count to within normal limits.
After three months on apixaban, Ms. B’s neurologist felt comfortable discontinuing anticoagulation, and she continues with aspirin 81 mg/day as thrombosis prophylaxis. After the apixaban was discontinued, a bone marrow aspiration and biopsy was pursued, and results were consistent with essential thrombocythemia: the marrow was normocellular (50%) without the presence of reticulin fibrosis. Ms. B continues on hydroxyurea, which has been titrated to achieve platelet control while avoiding leukopenia and anemia.
Discussion
Ms. B’s presentation highlights the importance of multidisciplinary collaboration, as co-managed care between neurology and hematology was critical for overall treatment success and safety. Initially, the etiology for Ms. B’s stroke was thought to be secondary to a hypercoagulable state in the setting of recent COVID infection. In the past two years, we have seen a high relative incidence of vascular events, including thrombosis, soon after COVID-19 diagnosis, which can remain elevated for up to 49 weeks.1 Thrombocytosis in the setting of infection and inflammation can certainly be reactive; however, investigating for a primary bone marrow etiology is important for comprehensive assessment and appropriate management.
Reference
- Knight R, et al. Association of COVID-19 With Major Arterial and Venous Thrombotic Diseases: A Population-Wide Cohort Study of 48 Million Adults in England and Wales. Circulation. 2022;146:892-906.