Patient With Post-PV Myelofibrosis–Related Anemia
Presentation
Mrs. N is a 73-year-old female with post-PV myelofibrosis, diagnosed in 2008. Her past medical history is significant for chronic liver disease, portal vein thrombosis, and subsequent partial small bowel resection, portal hypertension, and esophageal varices. She has been treated for myelofibrosis with multiple agents in the past, including enrollment on a number of clinical trials. Mrs. N was most recently taken off a clinical trial due to lack of efficacy, and she remains on low-dose ruxolitinib due to thrombocytopenia and anemia.
Disease Classification (DIPSS Plus)1
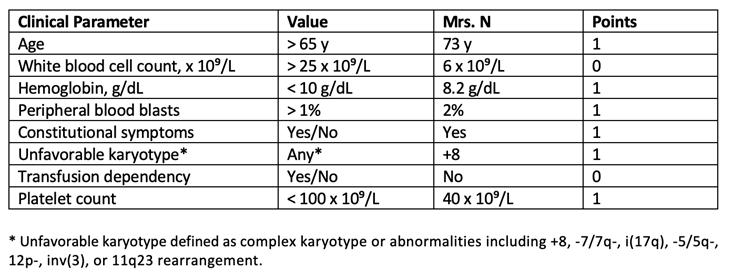
Mrs. N has high-risk disease based on DIPSS Plus scoring for age, hemoglobin, peripheral blasts, constitutional symptoms, unfavorable karyotype, and thrombocytopenia. Her most recent bone marrow biopsy showed persistent myeloproliferative neoplasm/myelofibrosis, overt fibrotic stage, and no increase in blasts. Myeloid next-generation sequencing showed persistent mutations in ASXL1, TET2, and JAK2. Cytogenetics: 48,XX,+8,+9[15]/46,XX[5].
Progression of Anemia
Recently, Mrs. N started needing occasional red blood cell transfusion support, and current efforts are being made to try and reduce the frequency and possibly eliminate the need for packed red blood cell transfusions. A full workup to evaluate for possible contributing causes of her anemia revealed iron deficiency, which was repleted with a dose of intravenous iron. B12 and folate were within normal limits. Mrs. N has no chronic kidney disease, and erythropoietin was appropriate at 412. After the iron deficiency was corrected, her hemoglobin did improve for a few months. Unfortunately, despite normal iron levels, her hemoglobin dropped again, and Mrs. N started experiencing more fatigue, which she relates to her anemia.
Potential treatment options were discussed with Mrs. N, and unfortunately, due to living out of state, traveling for a clinical trial at our center was not desirable for her at this time. She started taking danazol 200 mg BID and did so for 3 months, at which time there was no improvement; danazol was then discontinued. Years prior, Mrs. N had been on a clinical trial with sotatercept and had had a good response. The advanced practitioner on the treatment team discussed with her that luspatercept, an agent very similar to sotatercept, was now an option; she decided to proceed. Mrs. N has continued ruxolitinib due to its persistent positive effect on controlling splenomegaly.
Luspatercept Initiation2
Mrs. N has reviewed the potential risks/benefits and dosing of luspatercept with the clinical pharmacist. She is willing to come to town every 3 weeks for the injection with the understanding that there are important dose modifications that may need to take place to elicit the maximum response. The starting dose is 1 mg/kg, with dose escalation to 1.33 mg/kg if she is not transfusion-free after at least 2 consecutive doses at 1 mg/kg, and again to 1.75 mg/kg if she still is not transfusion-free after at least 2 doses of 1.33 mg/kg. Blood pressure is monitored closely, as this is a known possible adverse event. Mrs. N’s hemoglobin is 7.1 g/dL at the time of dose 1. A complete blood count check 12 days later showed an increase in hemoglobin to 9.8 g/dL without transfusion support. She is very pleased with the improvement, and will continue the current dosing strategy for now, with dose 2 planned for the next week.
Discussion
At some point, nearly all patients with myelofibrosis will develop anemia either as a result of the disease itself or as a treatment-related side effect. Eventually, most patients will require RBC transfusions, and some may become transfusion dependent. Unfortunately, dependence on RBC transfusions is one risk factor associated with inferior survival.3 It is important to rule out other common causes of anemia as they may co-exist, especially in our patient population, typically in their sixth or seventh decade of life. Emerging therapies offer hope for patients; it is important for advanced practitioners to be up to date on novel therapies and how to implement them in clinical practice.
References
- 1. Gangat N, et al. DIPSS plus: A refined Dynamic International Prognostic Scoring System for primary myelofibrosis that incorporates prognostic information from karyotype, platelet count, and transfusion status. J Clin Oncol. 2011;29:392-397.
- 2. NCCN Clinical Practice Guidelines in Oncology. Myeloproliferative Neoplasms. Version 2.2021 Published August 18, 2021. Accessed February 8, 2022. https://www.nccn.org/professionals/physician_gls/pdf/mpn.pdf
- 3. Chifotides HT, et al. Momelotinib: An emerging treatment for myelofibrosis patients with anemia. J Hematol Oncol.2022;15:7.