Classical Case of Essential Thrombocythemia: Diagnosis and Management
Presentation
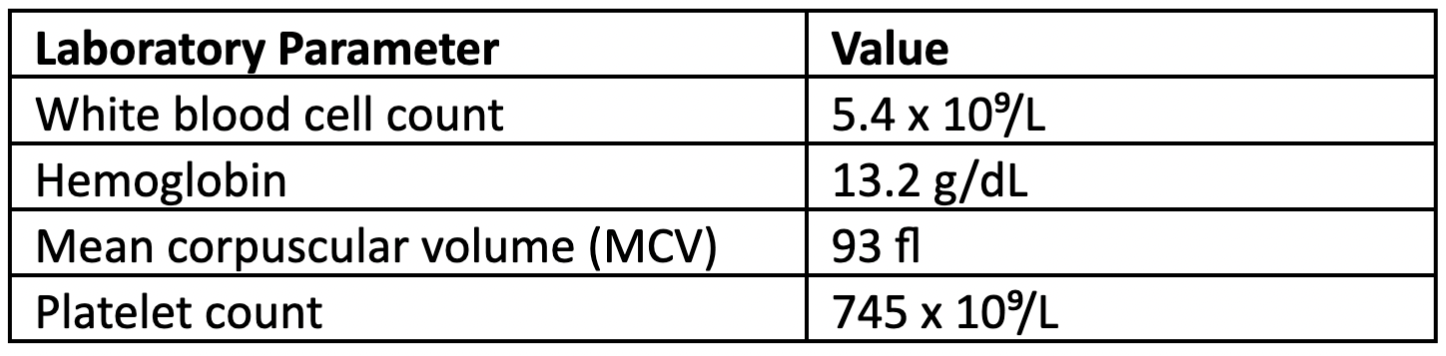
A 63-year-old female with hypertension and hypercholesterolemia presented to the hematology clinic after routine lab work at a local health fair revealed elevated platelets. The patient brought the lab results with her, which revealed the following pertinent complete blood count (CBC) values:
The patient presented in her usual state of health and was not having any symptoms concerning to her aside from anxiety about the high platelet count. She reported that her blood pressure was well controlled on her current antihypertensive regimen, and she had managed her high cholesterol with diet and exercise. She reported no history of iron deficiency or recent noticeable blood loss. She denied having any recent surgeries, acute infection at the time of the lab draw, or symptoms consistent with possible autoimmune process. Importantly, the patient denied history of a thrombotic event.
Workup
Physical exam was unremarkable. Notably, there was no palpable splenomegaly.
Repeat CBC was consistent with a normal white blood cell differential and isolated thrombocytosis with a platelet count of 725 x 10⁹/L. Despite a normal MCV, a full iron panel to rule out iron deficiency as the etiology for thrombocytosis was obtained. This was unremarkable with ferritin, iron saturation, transferrin, and serum iron all within normal limits (WNL). Lactate dehydrogenase was WNL.
Bone marrow aspiration and biopsy was performed for better classification of the likely underlying myeloproliferative neoplasm:
- Bone marrow morphology: normocellular marrow with increased number of enlarged, megakaryocytes with no significant increase in neutrophil granulopoiesis or erythropoiesis. No fibrosis. No evidence of dysplasia. No increase in CD34+ blasts by flow cytometry.
- Diploid karyotype
- Molecular panel sent on the bone marrow aspirate identifying JAK2 V617F mutation
- No additional mutations identified, including a negative BCR/ABL
Treatment
Based on these results, the patient was informed that she had a diagnosis of essential thrombocythemia (ET) with a JAK2 mutation. She was recommended to start cytoreductive therapy due to her being older than age 60 to reduce the risk of thrombotic or bleeding events. Interferon or hydroxyurea were proposed as front-line agents, and the patient decided to pursue treatment with hydroxyurea. Additionally, she was instructed to start low-dose aspirin (81 mg/day).
The patient was advised to continue close follow-up with her primary care provider for optimal management of hypertension, hypercholesterolemia, and cardiovascular risk factors. Additionally, she was referred to a dermatologist as treatment with hydroxyurea does place her at increased risk for the development of non-melanoma skin cancers.
Discussion
This case represents a classic presentation of a patient with a new diagnosis of JAK2+ ET. Additional mutations commonly seen in ET include CALR and MPL; however, these three driver mutations are mutually exclusive and will not co-occur. It is important to note that the dose of hydroxyurea was titrated a number of times within the first six months of treatment in order to achieve normal platelet count, while at the same time avoiding the development of anemia or neutropenia. Initial management of patients with ET on cytoreductive therapy may require more frequent visits and lab tests until the optimal dose is established. Longer-term follow-up is necessary for continued CBC monitoring for disease control on the current therapy and any clinical or laboratory changes indicating potential transformation to myelofibrosis. Evaluation for the presence of symptoms or the development of splenomegaly is also an important part of follow-up for patients with ET.
Of note, the 2016 WHO revised classification and diagnosis of ET includes a bone marrow evaluation. The purpose is to differentiate between ET and prefibrotic myelofibrosis, both of which may present with an isolated thrombocytosis on laboratory studies. Median survival is significantly shorter in prefibrotic myelofibrosis than ET, and therefore having appropriate diagnosis is critical for optimal monitoring and management.1,2
References:
- Barbui T, et al. The new WHO classification for essential thrombocythemia calls for revision of available evidences. Blood Cancer J. 2020;10:22.
- Thiele J, et al. Essential thrombocythemia versus early primary myelofibrosis: a multicenter study to validate the WHO classification. Blood 2011;117:5710-5718.