Sclerodermatous Chronic GVHD
Presentation and Diagnosis
A 27-year-old female presents for long-term follow-up and care of her chronic graft-vs-host disease (GVHD). She has a past medical history of refractory acute lymphoblastic leukemia (ALL) diagnosed at age 18. She underwent a matched sibling donor (brother) allogeneic stem cell transplant at age 20 using a busulfan/cyclophosphamide/total body irradiation conditioning regimen. Her GVHD prophylaxis included mycophenolate mofetil days 5–35 post-transplant, as well as tacrolimus. Her post-transplant course was relatively unremarkable with the exception of expected cytopenias and gastrointestinal symptoms. Tacrolimus was tapered between days 100 and 180. The patient did not have a history of acute GVHD. She was confirmed to be in minimal residual disease–negative remission for her ALL at day 100 and at 1 and 2 years post-transplant bone marrow biopsies. She is currently approximately 7 years post-transplant at the time of initial presentation.
At her initial consultation, she reports that she has been dealing with recently worsening symptoms of GVHD. She reports no recent infections, but she was hospitalized last year for sepsis/pneumonia and has fully recovered without any lung symptoms. She reports she had a recent pulmonary function test that was relatively normal.
From a symptom perspective, she reports sensitivity to acidic and spicy foods. She reports sicca syndrome with symptoms of dry eyes. She also developed mouth dryness. The patient reports tightness in her skin and joints, as well as pain in her back during recent months and leg, foot, and hand cramping.
Due to high-dose steroid use before transplant as part of her induction regimen, she developed avascular necrosis of the bilateral hips and also was found to have osteopenia on a recent DEXA scan. She has a history of femur fracture, which is now healed. The patient works in the medical field and retains impressive functionality despite her symptoms.
The following are the results of her systematic GVHD assessment1:

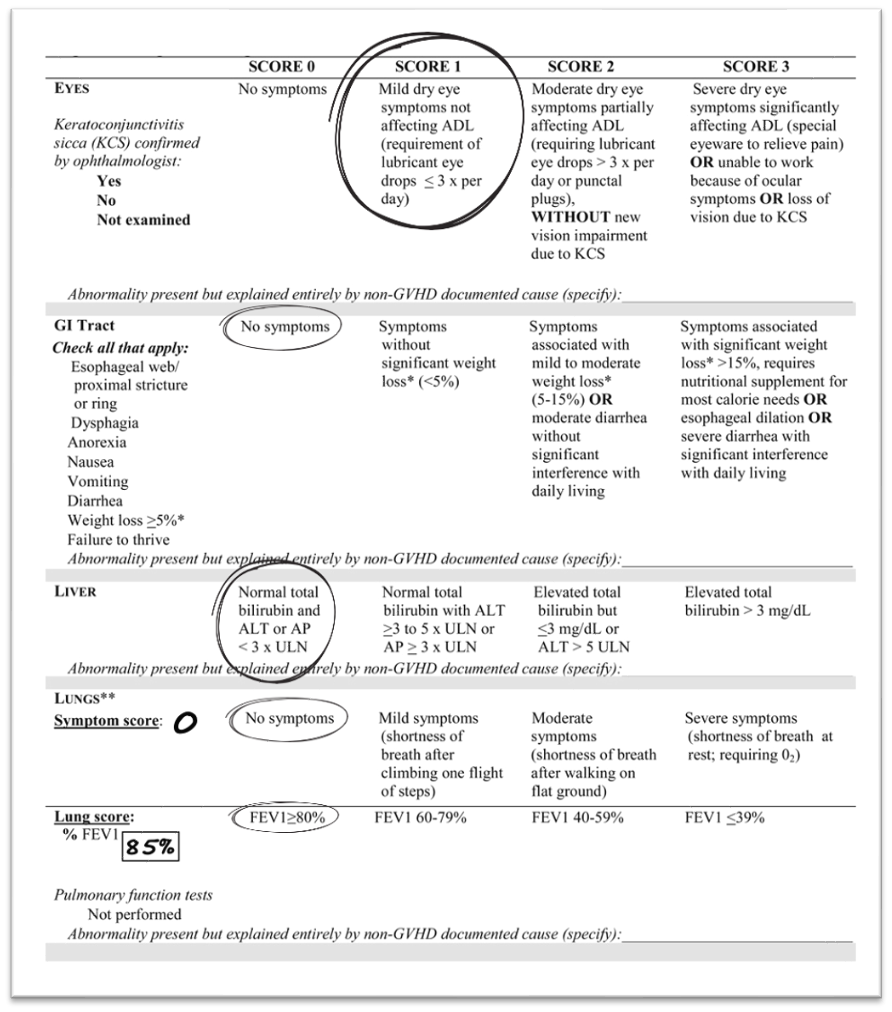

A focused physical exam finds the following:
- Mild scleral injection/erythema and photophobia
- Lichenoid changes with mild erythema in the bilateral buccal mucosa
- Limited range of motion in her elbows and shoulders
- Skin exam reveals sclerodermatous changes on the bilateral biceps, forearms, shoulders, and thighs.
- Dimpling and fascial tightness and some hyper and hypopigmentation on the skin, which is firm but movable
The patient is currently taking Systane lubricating eye drops (1 drop in each eye, as needed for eye dryness) and citalopram 20 mg by mouth daily. Also included in her medication list is ruxolitinib 5 mg twice daily; the patient reports this has been prescribed but not yet approved by insurance at the first visit.
Her labs at the time of initial evaluation:

Treatment
When a patient is found to have moderate chronic GVHD on assessment, it is apparent that they need systemic treatment. However, due to this patient’s previous high-dose steroid use and unfortunate development of avascular necrosis of the bilateral hips, osteopenia, and history of femur fracture, the use of steroids is questionable, if not prohibited. The patient declined the use of further steroids due to her bone history, but insurance did not want to approve the use of ruxolitinib without the failure of steroids.2,3 An appeal letter was sent to the insurance company and ruxolitinib was eventually approved.
Following approximately 4 weeks on ruxolitinib at 10 mg twice daily, the patient reported stable symptoms. She also reported increased symptoms of short-term memory loss and difficulty completing tasks as a medical professional at work. She cited a few examples of her inability to recall numbers or doses of medications when tasked with medication administration. After 6 weeks on ruxolitinib, she opted to self-discontinue the medication.
The patient was prescribed ibrutinib 420 mg daily4 and reported some improvement in her elbow and knee tightness and range of motion after approximately 6 weeks. However, the dose was reduced to 280 mg daily due to nausea and increased cramping thought to be attributable to ibrutinib.5 She continued ibrutinib at the lower dose for several months until she experienced a plateau in improvement and increasing bone and muscle pain. She then was switched to belumosudil at 200 mg daily.6 Following 4 weeks of treatment, she was noted to have improvement in joint and bone pain off ibrutinib and some minor improvements in her range of motion. Mouth and skin scores both improved to 0 and 1, respectively. She continues on belumosudil at this time.
Discussion
For patients with a history of steroid toxicities—such as avascular necrosis, osteopenia or osteoporosis, pathologic fractures, uncontrolled diabetes, or other side effects—steroids should be minimized and avoided where possible. In this patient’s case, appeal to insurance allowed approval of systemic ruxolitinib without her being steroid-refractory. Ruxolitinib was not tolerated in this patient’s case, but her symptoms of short-term memory loss were unusual and not common in patients reporting neurologic complications. Ruxolitinib adverse reactions include dizziness (15%–18%), fatigue (13%), and headache (15%).7 This patient also had adverse effects with ibrutinib, and her symptoms were more commonly reported by other patients who have taken ibrutinib, with up to 25% reporting nausea and up to 36% reporting musculoskeletal pain.7
This case underscores the importance of having multiple options for the treatment of chronic GVHD and the limitations and toxicity of long-term steroids. Additional treatment options with better toxicity profiles may also be helpful in the future. This patient has been on all three FDA-approved options for chronic GVHD (ibrutinib, ruxolitinib, and belumosudil).8 Sclerodermatous changes are some of the most difficult symptoms for patients because they can be irreversible due to the sclerosis or scarring. In the past, stopping the progression of the scleroderma was the goal of treatment. With newer agents, improvement and reversal of sclerodermatous changes are possible and a hopeful turn to the future of understanding the pathways of scar tissue development. Of note, one nonmedical option for these patients is deep myofascial massage, which can help to improve or maintain range of motion in patients with fasciitis or scleroderma.9
References
- Jagasia MH, Greinix HT, Arora M, et al. National Institutes of Health Consensus Development Project on Criteria for Clinical Trials in Chronic Graft-versus-Host Disease: I. The 2014 Diagnosis and Staging Working Group report. Biol Blood Marrow Transplant. 2015;21:389-401.e1.
- US Food and Drug Administration. FDA approves ruxolitinib for chronic graft-versus-host disease. September 22, 2021. Accessed November 28, 2023. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-ruxolitinib-chronic-graft-versus-host-disease
- Le RQ, Wang X, Zhang H, et al. FDA Approval Summary: Ruxolitinib for Treatment of Chronic Graft-Versus-Host Disease after Failure of One or Two Lines of Systemic Therapy. Oncologist. 2022;27:493-500.
- US Food and Drug Administration. FDA expands ibrutinib indications to chronic GVHD. August 2, 2017. Accessed November 28, 2023. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-expands-ibrutinib-indications-chronic-gvhd
- Doki N, Toyosaki M, Shiratori S, et al. An Open-Label, Single-Arm, Multicenter Study of Ibrutinib in Japanese Patients With Steroid-dependent/Refractory Chronic Graft-Versus-Host Disease. Transplant Cell Ther. 2021;27:867.
- Przepiorka D, Le RQ, Ionan A, et al. FDA Approval Summary: Belumosudil for Adult and Pediatric Patients 12 Years and Older with Chronic GvHD after Two or More Prior Lines of Systemic Therapy. Clin Cancer Res. 2022;28:2488-2492.
- Wolters Kluwer. Lexicomp: Evidence-Based Drug Referential Content. 2023. https://www.wolterskluwer.com/en/solutions/lexicomp
- Zeiser R, Lee SJ. Three US Food and Drug Administration-approved therapies for chronic GVHD. Blood. 2022;139:1642-1645.
- Flowers ME, Martin PJ. How we treat chronic graft-versus-host disease. 2015;125:606-615.