Acute Skin GVHD and CMV Reactivation
Initial Diagnosis and Treatment
A 60-year-old male presented with myelodysplastic syndrome (MDS) with a Revised International Prognostic Scoring System (IPSS-R) score of 5.5 (i.e., high-risk disease) due to low hemoglobin, low platelets, and poor risk cytogenetics. Following treatment with 5 cycles of azacitidine, he moved forward with a matched unrelated allogeneic hemopoietic cell transplant using peripheral blood source, and he was conditioned with fludarabine and melphalan. The patient and donor were ABO mismatched (donor A+, recipient O+), and while the patient was cytomegalovirus (CMV) seropositive, the donor was CMV seronegative. Both recipient and donor were Epstein-Barr virus (EBV) seropositive.
Graft-vs-host disease (GVHD) prophylaxis consisted of post-transplant cyclophosphamide, tacrolimus, and mycophenolate mofetil (MMF) through day +35. The patient experienced white cell engraftment around day +18 and platelet engraftment around day +25. MMF was discontinued around day +35. Early post-transplant course was relatively unremarkable. Due to serostatus, the patient was monitored for CMV and EBV weekly with polymerase chain reaction (PCR) testing. Letermovir was used for CMV prophylaxis for the first 100 days.¹ Peripheral blood chimerism at day +30 revealed >98% donor chimerism, and there was no detectable recipient DNA.
The patient developed an erythematous, raised maculopapular rash around day +49.
GVHD Workup, Grading, and Staging
The rash was on the patient’s chest (9%), upper back (9%), lower back (9%), abdomen (9%), and anterior bilateral arms (4.5% x 2 = 9%), as well as his upper posterior arms/shoulders bilaterally (approx. 2.5 x 2 = 5%). Total involvement was approximately 51% and spared the buttocks, abdomen, bilateral legs, neck, and face. A skin punch biopsy revealed the likelihood of acute GVHD. Clinically, the patient was diagnosed with acute GVHD of the skin stage 3.
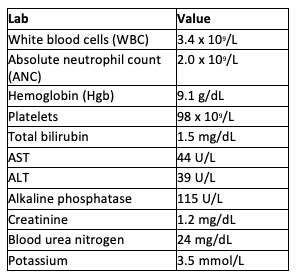
At the time, bilirubin was 1.5, aspartate transaminase (AST) and alanine transaminase (ALT) were slightly above normal limits, and the patient reported no diarrhea, overall clinical grade II.² The tacrolimus was therapeutic at a level of 8. The rest of the patient’s blood counts were stable:
ST2 and Reg3α were measured according to the Acute GVHD Symptomatic Onset Algorithm, and the ratio put the patient in a low-risk category for non-relapse mortality.
GVHD Treatment Initiation
Following the punch biopsy, the patient was started on prednisone at 1 mg/kg/day in divided doses (the patient was approximately 100 kg, so he split 60 mg in the morning and 40 mg in the early evening). He continued on therapeutic tacrolimus. The rash improved within approximately 1 week of beginning high-dose steroids.
CMV Reactivation
CMV PCR at the time of initiation of steroids had remained negative, but following 2 weeks on steroids, the patient began to have CMV viremia, which was detected at 1400 IU/mL.
For the first week, letermovir continued, but CMV PCR increased to 3127 IU/mL. Letermovir was discontinued, and the patient was started on valganciclovir 900 mg twice daily x 14 days. Following the initiation of valganciclovir, the blood counts dropped due to myelosuppression associated with this medication.

CMV PCR following 1 week of valganciclovir was 1236 IU/mL, and after 2 weeks, it was down to detected non-quantifiable. The patient was switched to maintenance dose valganciclovir at 450 mg twice daily until two negative CMV PCR tests. The patient was monitored and did not develop any symptom of CMV disease despite detectable CMV viremia.
GVHD Response
Prednisone was tapered quickly over the following weeks (60 mg morning and 20 mg evening x 1 week, then 40 mg morning and 20 mg evening x 7 days, then 40 mg morning only), but the patient’s rash recurred after tapering below 0.5 mg/kg. At that time, he was initiated on ruxolitinib 5 mg twice daily for 3 days and increased to 10 mg twice daily because he did not experience toxicity. GVHD improved over the following 10-14 days. Steroids were able to be successfully tapered, while the patient continued ruxolitinib 10 mg twice daily.³ Letermovir was reinitiated following discontinuation of maintenance valganciclovir.
The 100-day workup revealed that the patient was in remission, with >98% donor chimerism in the peripheral blood and bone marrow samples.
Discussion
Patients with a history of seropositivity for CMV prior to transplant have a risk of reactivation following allogeneic stem cell transplantation. CMV viremia carries the risk of CMV disease, where the virus infiltrates the tissue and causes damage (commonly in the lungs and colon but also in other areas of the body such as the eyes, brain, and other tissues).Donor serostatus has been a controversial issue, but studies suggest patients who are seropositive carry better long-term outcomes.⁵ In recent years, it has become more standard practice to offer letermovir prophylaxis for seropositive recipients.¹ Because this patient had high-risk IPSS-R MDS and his donor options were limited, a donor who was unrelated and CMV seronegative and had major ABO mismatch was chosen for him. This may have contributed to his risk for both GVHD and CMV reactivation.
In this patient, despite letermovir prophylaxis, the initiation of high-dose steroids allowed breakthrough CMV viremia. Valganciclovir is an oral option instead of intravenous ganciclovir. Regrettably, the treatment of CMV reactivation with valganciclovir or ganciclovir both often result in worsening cytopenias or pancytopenia. If this patient had developed CMV disease, additional treatment options may have also included CMV-specific T-cell infusion.⁶ Because this patient’s GVHD biomarkers of ST2 and Reg3α predicted lower risk for GVHD-related complications, the provider was more confident in a rapid taper of steroids.⁷˒⁸ However, the recurrence of rash following the taper suggested the need for a second agent. Ruxolitinib is FDA approved in acute GVHD for patients who have glucocorticoid-refractory acute GVHD.⁹
References
- Marty FM, Ljungman P, Chemaly RF, et al. Letermovir prophylaxis for cytomegalovirus in hematopoietic-cell transplantation. N Engl J Med. 2017;377:2433-2444.
- Harris AC, Young R, Devine S, et al. International, multicenter standardization of acute graft-versus-host disease clinical data collection: A report from the Mount Sinai Acute GVHD International Consortium. Biol Blood Marrow Transplant. 2016;22:4-10.
- Zeiser R, von Bubnoff N, Butler J, et al. Ruxolitinib for glucocorticoid-refractory acute graft-versus-host disease. N Engl J Med. 2020;382:1800-1810.
- Ljungman P, Brand R, Einsele H, et al. Donor CMV serologic status and outcome of CMV-seropositive recipients after unrelated donor stem cell transplantation: an EBMT megafile analysis. 2003;102:4255-4260.
- van Kraaij MG, Verdonck LF, Rozenberg-Arska M, et al. Early infections in adults undergoing matched related and matched unrelated/mismatched donor stem cell transplantation: A comparison of incidence. Bone Marrow Transplant. 2002;30:303-309.
- Kaeuferle T, Krauss R, Blaeschke F, et al. Strategies of adoptive T -cell transfer to treat refractory viral infections post allogeneic stem cell transplantation. J Hematol Oncol. 2019;12:13.
- Major-Monfried H, Renteria AS, Pawarode A, et al. MAGIC biomarkers predict long-term outcomes for steroid-resistant acute GVHD. 2018;131:2846-2855.
- Eurofins Viracor. aGVHD Pre-Symptomatic Algorithm. Accessed January 28, 2024. https://www.eurofins-viracor.com/clinical/test-menu/403571p-agvhd-pre-symptomatic-algorithm/
- US Food and Drug Administration. FDA approves ruxolitinib for acute graft-versus-host disease. Published May 24, 2019. Accessed January 28, 2024. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-ruxolitinib-acute-graft-versus-host-disease