Bone Protection During Chemotherapy in Metastatic Lung Cancer
Presentation
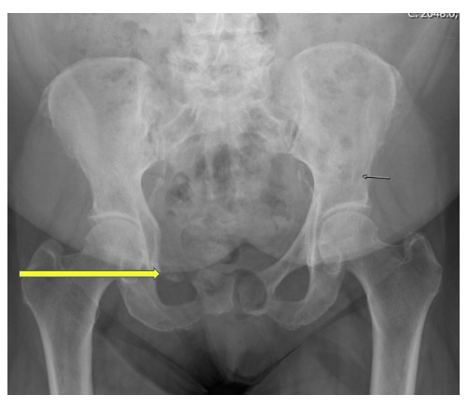
A 72-year-old African American woman with non-small cell lung cancer (NSCLC) experiences recurrence of her disease. At the time of recurrence, she has significant pain in her right hip and groin area and is not able to move about well. In fact, she has to use a wheelchair to travel any sort of walking distance. The x-ray of her pelvis seen below reveals a large lytic lesion in the right superior pubic ramus, as well as acetabulum with periosteal reaction and a linear lucency that is indicative of a pathologic fracture.
Workup
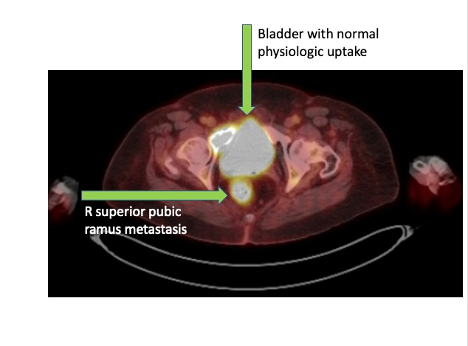
The patient sees an orthopedic surgeon who determines that surgery is not needed at this time. A positron emission tomography (PET) with 18-fluorodeoxyglucose (FDG) scan shows that the cancer has spread into her hip and groin region and has completely obliterated her right pubic ramus, which the x-ray had already indicated. Given her age and disease stage, she faces increased risk of skeletal-related events (SREs) on an already painful, weight-bearing bone.
Treatment and Management
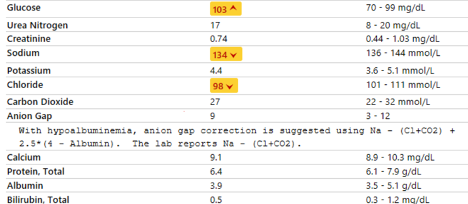
The patient starts on pemetrexed 500 mg/m2 and carboplatin AUC 5 for her metastatic NSCLC. To reduce her risk for SREs associated with bone metastases, she is given the bisphosphonate zoledronic acid at a dose of 4 mg intravenously on a monthly basis. Her baseline lab results reveal good renal function and stable calcium levels. She is given 600 mg of calcium and vitamin D orally twice a day.
Discussion
Newer therapies are extending survival in NSCLC, but the chance of developing bone metastases increases as a patient grows older and lives longer with the disease. Bone metastases can cause SREs, which in the case of this patient could have been a fracture in her hip and pelvis.
Zoledronic acid is a bisphosphonate that can reduce the incidence of SREs in cancer patients. It is approved by the U.S. Food and Drug Administration for treating metastatic bone disease in multiple cancers, including lung cancer, based on data from phase III trials for zoledronic acid.1,2
Zoledronic acid is generally administered every 4 weeks to reduce the incidence of SREs in patients with metastatic lung cancer. However, a study published in 2020 found that NSCLC patients with bone metastases who received zoledronic acid every 12 weeks had similar incidences of SREs after one year.3
Certain therapies that are used to treat osteoporosis, Paget’s disease, and other bone conditions can reduce the incidence of SREs in cancer patients. Pamidronate was one of the first, and zoledronic acid and denosumab are the two most commonly used today. Denosumab, an anti-RANKL drug, and zoledronic acid are newer-generation agents with less toxicity and more desirable dosing strategies. Both are associated with excellent protection against SREs.
While determining the optimal dosing of zoledronic acid in metastatic lung cancer is a fluid process, clinicians currently reduce the standard dose if a patient has renal insufficiency. Another option—either at this point or earlier, at the time of initiation of bone-modifying agent therapy—would be to consider denosumab, which does not require dose modification for renal insufficiency. Denosumab would be dosed at 120 mg by subcutaneous injection every 4 weeks. In patients who do have renal insufficiency, it is especially important to monitor for hypocalcemia, as the risk of this side effect increases when receiving denosumab in the setting of renal compromise.4
References
- Rosen, LS, Gordon, D, Tchekmedyian, S,et al. Zoledronic acid versus placebo in the treatment of skeletal metastases in patients with lung cancer and other solid tumors: a phase III, double-blind, randomized trial—the Zoledronic Acid Lung Cancer and Other Solid Tumors Study Group. J Clin Oncol.2003; 21:3150-3157. doi:10.1200/JCO.2003.04.105
- Rosen, LS, Gordon, D, Tchekmedyian, NS, et al. Long-term efficacy and safety of zoledronic acid in the treatment of skeletal metastases in patients with non small cell lung carcinoma and other solid tumors. Cancer. 2004; 100:2613-2621. doi:10.1002/cncr.20308
- Tam AH, Schepers AJ, Qin A, Nachar VR. Impact of extended-interval versus standard dosing of zoledronic acid on skeletal events in non–small-cell lung cancer and small-cell lung cancer patients with bone metastases.Annals of Pharmacotherapy. 2021;55(6):697-704. doi:10.1177/1060028020967629
- Jalleh R, Basu G, Le Leu R, Jesudason S. Denosumab-induced severe hypocalcaemia in chronic kidney disease. Case Rep Nephrol. 2018 Nov 4;2018:7384763. doi:10.1155/2018/7384763