Management of Adverse Effects in Patients With Multiple Myeloma Treated With Bispecific Antibodies
Haleigh Mistry,1 MS, PA-C, Beth Faiman,2 PhD, MSN, APN-BC, BMTCN, FAAN, FAPO, and Mikhaila Rice,3 PharmD, BCPS, BCOP
From 1Department of Lymphoma & Myeloma, MD Anderson Cancer Center, Houston, Texas; 2Department of Hematologic Oncology and Blood Disorders, Taussig Cancer Institute, Cleveland, Ohio; 3Department of Pharmacy, Cleveland Clinic, Cleveland, Ohio
Authors’ disclosures of conflicts of interest are found at the end of this article.
Correspondence to: Beth Faiman, PhD, MSN, APN-BC, BMTCN, FAAN, FAPO, Department of Hematologic Oncology and Blood Disorders, Taussig Cancer Institute, Cleveland, Ohio. E-mail: faimanb@ccf.org
Introduction
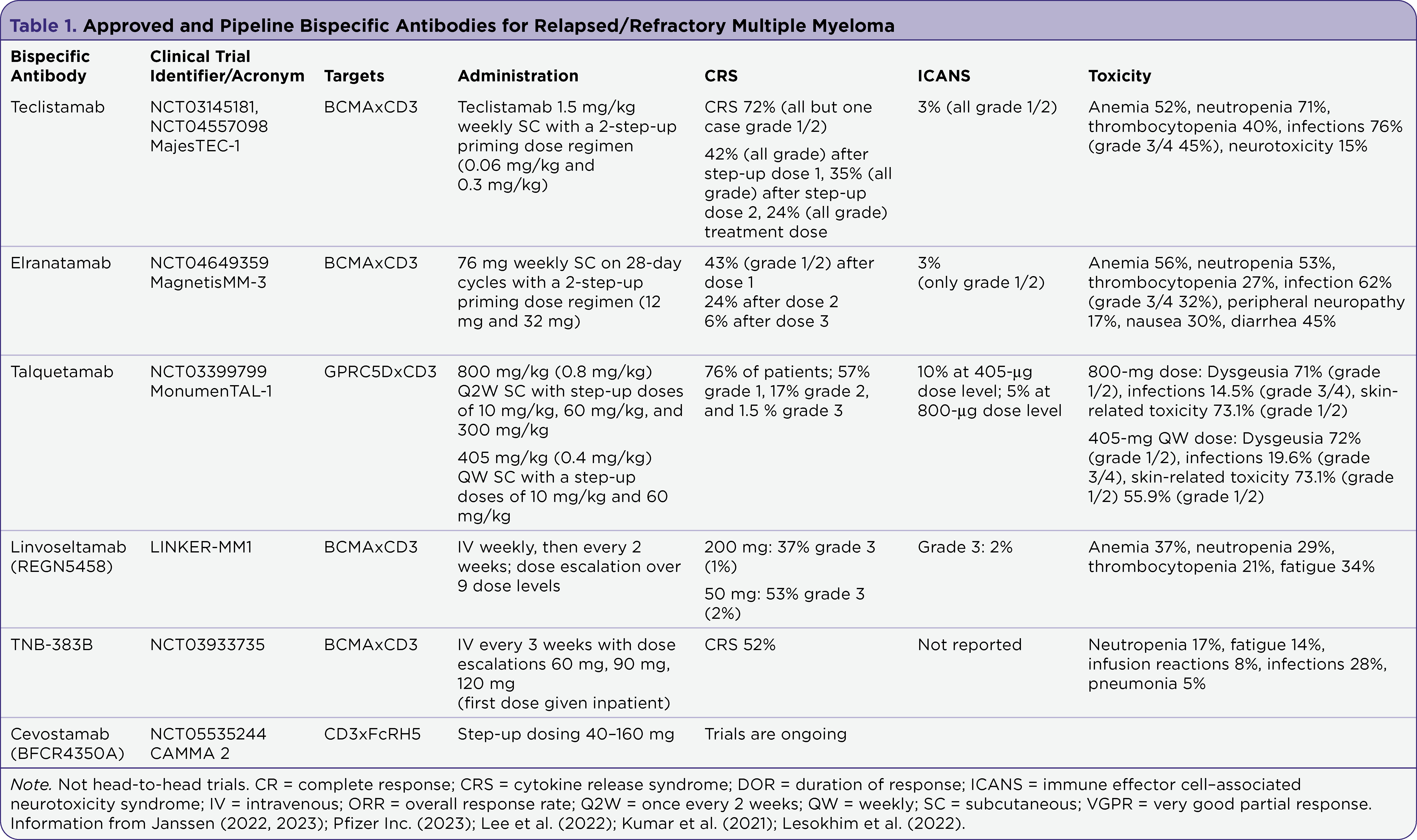
While therapies for multiple myeloma have dramatically advanced in recent years, patients with multi-drug resistant disease still have much less favorable outcomes. For patients with RRMM, BsAbs represent a new treatment option, with several now approved by the US Food and Drug Administration (FDA) and more in development (Table 1). BsAbs bind to tumor antigens along with CD3 on T cells, leading to T-cell activation and tumor death. Currently, there are three FDA-approved BsAbs for the treatment of relapsed or refractory multiple myeloma (RRMM).
Teclistamab, a T-cell–redirecting BsAb targeting both CD3 and B-cell maturation antigen (BCMA) expressed on the surface of myeloma cells, is the first BsAb FDA approved for the treatment of triple-class-exposed refractory multiple myeloma (Moreau et al., 2022). Common adverse events included cytokine release syndrome (CRS), immune effector cell–associated neurotoxicity syndrome (ICANS), cytopenias, and infections.
Talquetamab, another BsAb recently approved for treatment of RRMM, targets CD3 and G protein-coupled receptor, family C, group 5, member D (GPRC5D). In addition to CRS, ICANS, and infectious risk, talquetamab may cause unique adverse effects related to binding of GPRC5D, including skin, nail, hair, and mouth toxicity (Chari et al., 2022).
Lastly, elranatamab, most recently granted accelerated approval by the FDA, also targets BCMA and CD3, but differs from teclistamab in that it involves fixed-dose rather than step-up dosing. This article will describe common adverse effects with BsAb therapies, when they are expected to occur, and how they may be managed.
Cytokine Release Syndrome
Cytokine release syndrome (CRS) is an acute inflammatory syndrome characterized by fever, capillary leak contributing to hypoxia and hypotension, and subsequently organ dysfunction. CRS occurs due to cytotoxic T-cell activation, which causes the release of inflammatory cytokines, most notably IL-6, IFN-γ, TNF-α, and IL-1 as well as IL-2 inhibitors (Figure 1; Lee et al., 2019; Martin et al., 2023). Incidence varies with the type of immunotherapy, but it is more commonly seen with CAR-T cell therapy and BsAbs. Symptoms are often progressive but must include fever at the onset (Lee et al., 2019) and typically mimic symptoms of infection (Table 2; Cosenza et al., 2021). Because patients are often neutropenic, ruling out infection is essential. Higher grades of CRS are characterized by worsening hypotension and hypoxia in addition to fever. Additionally, patients may experience myalgias, arthralgias, nausea, vomiting, skin rash, tachycardia, and disseminated intravascular coagulation. Rarely, acute cardiac dysfunction occurs but is usually reversible (Cosenza, Sacchi, & Pozzi, 2021). It is well documented that CRS can cause cardiac effects. These range widely, from tachycardia to hemodynamic instability and reduced cardiac function. The overall etiology is thought to be secondary to the release of cytokines, causing transient tissue damage. To aid in monitoring, cardiac enzymes such as troponin and pro-B-type natriuretic peptide (Pro-BNP) may be monitored, as well as EKG monitoring and echocardiograms when clinically indicated. In most cases, acute cardiac dysfunction is reversible with proper intervention (Shalabi et al., 2020). Grading of CRS is imperative to accurately determine severity and guide management (Lee et al., 2019; Martin et al., 2023; Table 3).

Figure 1. Pathophysiology of cytokine release syndrome. IFN-γ = interferon-gamma; TNF-α = tumor necrosis factor-alpha; IL = interleukin; CSF = colony-stimulating factor; MCP = monocyte chemoattractant protein. Adapted from Cosenza et al. (2021).


Management of CRS is directed at treating the symptoms and the underlying inflammatory cytokines. Interdisciplinary collaboration is essential to ameliorate severe outcomes and prevent fatalities (Cosenza et al., 2021). Patients experiencing CRS grade 1 and grade 2 toxicities are usually managed with antipyretics, fluids, and potentially antibiotics if there is concern for infection. As CRS progresses and becomes more severe, patients may require oxygen supplementation and/or vasopressors for hypotension (Cosenza et al., 2021). In addition to providing symptomatic management, steroids and cytokine inhibitors, such as the IL-6 inhibitor tocilizumab, may be used to directly mitigate cytokine response (Martin et al., 2023).
Steroids
Steroids are often used in the setting of CRS to suppress the excessive inflammatory response. However, the use of steroids is controversial (based on CAR-T studies) due to potential detrimental effects on amplification and persistence of T cells, and consequently CAR T-cell therapy efficacy. In patients who experience severe CRS, the use of corticosteroids may be required to ablate CAR-T cells and allow for hemodynamic stabilization (Cosenza et al., 2021).
Cytokine Inhibitors
IL-6 receptor inhibitors such as tocilizumab, a humanized monoclonal antibody that inhibits IL-6 binding to its receptor, have demonstrated efficacy in management of CRS. Tocilizumab was granted FDA approval in 2017 as first-line treatment for CAR T-cell-induced CRS (Le et al., 2018). In contrast to steroids, tocilizumab can mitigate CRS without significant loss of CAR-T cell activity. Siltuximab, another IL-6 inhibitor, has also been used off-label to manage CRS, particularly during periods of tocilizumab shortage. For patients in whom IL-6 inhibitors were not effective in alleviating CRS symptoms, other cytokine inhibitors such as the TNF-α inhibitors etanercept and infliximab have been used, with mixed results. Anakinra, IL-1R antagonist, has also been used with promising results. IFN-γ inhibitors are not used to manage CRS even though IFN-γ is consistently elevated in severe CRS. Because of its role in T-cell proliferation, it is not thought to be an ideal target (Cosenza et al., 2021).
While tocilizumab is not FDA approved for CRS related to BsAb therapy and is not included in teclistamab or talquetamab package inserts explicitly, it has been readily used in this setting in clinical trials and in real-world practice (Moreau et al., 2022; Chari et al., 2022).
Immune Effector Cell–Associated Neurotoxicity (ICANS)
Although not completely understood, the mechanism underlying immune effector cell–associated neurotoxicity syndrome (ICANS) observed with BsAb and CAR-T therapy points to the release of inflammatory cytokines secreted by macrophages and monocytes. These cytokines increase the permeability of the blood-brain barrier (BBB) and lead to its breakdown (Rees, 2022). Neurologic toxicity ranges from mild symptoms such as headache to severe symptoms such as confusion, delirium, aphasia, tremor, seizures, and rarely death (Cosenza et al., 2021). An early feature of ICANS is deterioration of handwriting as well as speech hesitancy, which may present as both expressive and or receptive (Rees, 2022). Patients may experience slowed speech, delayed word finding, and or difficulty with speech interpretation. Because ICANS is a clinical diagnosis, early identification is imperative. ICANS severity can progress quickly, and rarely can result in status epilepticus and fatal cerebral edema (Rees, 2022).
Management of ICANS consists of supportive care and corticosteroids (Rees, 2022). The recommended treatments for ICANS grade 2 or higher are dexamethasone or methylprednisolone (Seigler & Kenderian, 2020). However, there is no clinical consensus on recommendations of further treatments for patients who do not respond to high-dose steroids. Paradoxically, tocilizumab is not effective against severe ICANS, likely due to its inability or limited ability to penetrate the BBB (Cosenza et al., 2021), and may worsen ICANS symptoms (Seigler & Kenderian, 2020). Therefore, tocilizumab use is not recommended in patients with ICANS unless there is concurrent CRS.
Management of ICANS is based on grade, which is in turn determined by the immune effector cell encephalopathy (ICE) score (Table 4). This is a 10-point scale evaluating orientation, language, writing, and attention; the higher the number of points, the lower the grade of ICANS (Rees, 2022). ICE scoring should be performed at least twice daily by the clinical provider and/or caregiver on patients who received T-cell engager therapy (BsAb or CAR-T), allowing for the assessment of subtle cognitive changes. In most cases, ICANS symptoms will resolve within a week with treatment, although severe ICANS may lead to fatal intracerebral hemorrhage and/or cerebral edema (Seigler & Kenderian, 2020).

For patients with increased risk of seizures or who have seizures with ICANS, it is recommended to initiate levetiracetam with or without phenobarbital and/or lacosamide (Neelapu, 2019), consider benzodiazepines (for acute control), and consult neurology/neuro-oncology. Patients with known seizure disorders are not excluded from receiving BsAb therapy; however, they may require closer monitoring due to risk of increased seizures secondary to ICANS. Patients may need neuroimaging, EEG monitoring, and or lumbar puncture. For patients with cerebral edema, prompt treatment is required by lowering intracranial pressure by hyperventilation, hyperosmolar therapy with mannitol/hypertonic saline and/or neurosurgery consultation for consideration of ventriculoperitoneal shunt (Neelapu, 2019).
Teclistamab
In the MajesTEC-1 phase I/II trial, which led to FDA approval of teclistamab, a total of 165 patients were treated, 77.6% of whom had triple-class refractory disease. With a median follow-up of 14.1 months, the overall response rate (ORR) was 63%, with a complete response (CR) rate of 39.4%, and 26.7% were minimal residual disease–negative (MRD). MRD is typically assessed by examination of bone marrow using next-generation sequencing and multiparameter flow cytometry to look for the presence of residual myeloma cells. The median time to first response was 1.2 months and median time to best response was 3.8 months. CRS occurred in 72% of patients (50% grade 1, 21% grade 2, and 0.6% grade 3). The median time to onset of CRS was 2 days (range, 1–6 days). Median duration of CRS was also 2 days (range, 1–9 days). As patients continued with step-up dosing, the rate of CRS declined: 42% of patients experienced CRS on step-up dose 1, 35% on step-up dose 2, and 24% on initial treatment dose (Figure 2; Moreau et al., 2022).

Figure 2. Teclistamab recommended dosing. Adapted from Janssen (2022).
In the trial, 57% of patients had neurologic toxicities, most commonly headache (25%), motor dysfunction (16%), sensory neuropathy (15%), and encephalopathy (13%). As follow-up continued, 1 patient on trial experienced grade 4 seizure and 1 patient had fatal Guillain-Barré syndrome. Of these toxicities, 2.4% were grade 3/4 (Janssen Pharmaceuticals, 2022). ICANS was reported in 6% of patients, and 1.8% experienced recurrent ICANS, most frequently dysgraphia and confusional state. Due to the risk of ICANS, patients were instructed to refrain from driving or operating machinery for 48 hours after completion of step-up dosing and treatment dose. ICANS can occur concurrently with CRS, following resolution of CRS, or can occur in the absence of CRS (Janssen Pharmaceuticals, 2022).
Prior to initiating teclistamab, patients should be given a wallet card and provided ample education on potential adverse events, most notably ICANS and CRS. Patients should be educated on potential adverse events such as fever, hypoxia, chills, hypotension, tachycardia, headache, elevated liver enzymes, dyspnea, and confusion (Janssen Pharmaceuticals, 2022). The FDA has mandated that all providers who prescribe teclistamab are registered with the teclistamab Risk Evaluation and Mitigation Strategy (REMS) program, which is designed to ensure providers are informed about serious adverse effects, including CRS and ICANS.
Other pertinent adverse events associated with teclistamab include cytopenias, infection, hepatotoxicity, and other long-term adverse effects. These may increase risk of dosing delay, requiring patients to restart teclistamab step-up dosing. A multidisciplinary approach, incorporating services such as but not limited to infectious disease, cardiology, neurology, hepatology, nephrology, and dermatology, is often essential to mitigate severe toxicities and prevent potentially fatal outcomes (Smith & Venella, 2017).
Cytopenias
The most common grade 3/4 laboratory abnormalities (≥ 20%) in MajesTEC-1 were decreased lymphocytes, decreased neutrophils, decreased white blood cells, decreased hemoglobin, and decreased platelets (Janssen Pharmaceuticals, 2022). In addition to cytopenias related to teclistamab, many patients treated with teclistamab have poor marrow function and cytopenias at baseline given aggressive relapsed or refractory disease. While disease-related cytopenias may improve with treatment, patients may require transfusion support for anemia or thrombocytopenia. Weekly or twice weekly lab monitoring as well as transfusion appointments should be arranged during the first few months of treatment as needed. Neutropenia was seen in 84% of patients treated with teclistamab, with 56% grade 3/4. Febrile neutropenia was reported in 3% (Janssen Pharmaceuticals, 2022). Use of granulocyte colony-stimulating factor (G-CSF) is not recommended within 10 days of treatment initiation due to increased risk of CRS (Ayuketang & Jäger, 2022) but it may be incorporated into treatment after step-up dosing and first treatment dose are completed. Patients who are neutropenic should be monitored closely for fever or infection.
Infections
Infections are common in patients receiving teclistamab (77% of patients), and patients are often at increased risk due to immunocompromise or hypogammaglobulinemia related to both disease and prior myeloma-directed treatment (Mohan et al., 2022). Due to ongoing therapy with BsAbs, patients are at increased risk of B-cell aplasia, further compounding the risk for infections (Mohan et al., 2022). Providers should monitor IgG levels and consider IVIG administration when indicated. The three most common types of infections in MajesTEC-1 were urinary tract infection (11%), pneumonia (24%), and upper respiratory infections (28%). Opportunistic infections occurred in 30% of patients in the MajesTEC-1 trial, grade 3/4 infections in 35%, and fatal infections in 4.2% (Janssen Pharmaceuticals, 2022). Pneumocystis jiroveci pneumonia (PJP) occurred in 3.6% of patients. Infections may lead to multiple dosing delays and can be devastating to patient response and recovery, increasing symptoms of fatigue and contributing to overall deconditioning. Fevers are common and may be the first presenting sign of infection; however, they may also be present with CRS. For this reason, it is imperative to rule out infection when fever is present by performing cultures, chest X-ray, and urinalysis.
All patients on teclistamab should receive antiviral and PJP prophylaxis. Antibacterials, and antifungals should be added for patients who are neutropenic per provider discretion and institutional recommendations. Hepatitis B testing should be performed prior to treatment initiation, and prophylaxis to prevent reactivation should be provided in patients with a history of hepatitis B (Janssen Pharmaceuticals, 2022). Patients with signs of acute infection should be managed with appropriate antimicrobials, and infectious disease consult should be considered. Intravenous immunoglobulin (IVIG) may also be given prophylactically or to help manage opportunistic infections (Mohan et al., 2022).
Hepatotoxicity
In the MajesTEC-1 trial, 34% of patients had grade 1/2 elevated aspartate aminotransferase (AST), with 1.2% being grade 3/4. Grade 1/2 elevated alanine aminotransferase (ALT) occurred in 28% of patients, with 1.8% grade 3/4. Six percent of patients had elevated bilirubin, and one patient had fatal hepatic failure. This highlights the importance of reviewing a patient’s medications in detail as drug interactions or other medications may also lead to liver impairment. Patients may experience liver enzyme elevations with or without concurrent CRS (Janssen Pharmaceuticals, 2022).
Talquetamab
In the MonumenTAL-1 phase II trial, a total of 187 patients were treated, which included patients who had received at least four prior lines of therapy and who were not exposed to prior T-cell redirection therapy. CRS occurred in 76% of patients (57% grade 1, 17% grade 2, and 1.5 % grade 3). The median time to onset of CRS was 27 hours from last dose (range, 0.1–167 hours). Median duration of CRS was also 17 hours (range, 0–622 hours; Janssen Pharmaceuticals, 2023). As patients continued with step-up dosing, the rate of CRS declined: 29% of patients experienced CRS on step-up dose 1, 44% on step-up dose 2, 33% on step-up dose 3, and 30% on initial treatment dose (Figure 3; Chari et al., 2022).

Figure 3. Talquetamab (A) weekly and (B) biweekly dosing schedule. Adapted from Janssen (2023).
In the trial, 55% of patients had neurologic toxicities, most commonly headache (20%), encephalopathy (15%), sensory neuropathy (14%), and motor dysfunction (10%). Of these toxicities, 6% were grade 3/4. ICANS was reported in 9% of patients, with 3% experiencing recurrent ICANS. The most ICANS common symptoms seen with talquetamab included confusional state, depressed level of consciousness, disorientation, somnolence, lethargy, and bradyphrenia (Janssen Pharmaceuticals, 2023).
Prior to initiating talquetamab, patients should be given a wallet card and provided ample education on potential adverse events, most notably ICANS and CRS. They should also be registered through the Risk Evaluation and Mitigation Strategy (REMS) program. Patients should be educated on potential adverse events such as fever, hypoxia, chills, hypotension, tachycardia, headache, elevated liver enzymes, dyspnea, and confusion (Janssen Pharmaceuticals, 2023). The FDA has mandated that all providers who prescribe teclistamab are registered with the teclistamab REMS program, which is designed to ensure providers are informed about serious adverse effects, including CRS and ICANS.
Similarly to teclistamab, common adverse effects associated with talquetamab include cytopenias, infection, and hepatotoxicity. However, due to expression of GPRC5D in other tissue, most commonly hair follicle, nails, and tongue, talquetamab may cause additional adverse effects that could significantly impact patient’s quality of life (Chari et al., 2022; Verkleij et al., 2021).
Skin
Skin-related events occurred in 62% of patients. The most common skin-related adverse events included skin exfoliation, pruritus, and dry skin. Grade 3 and 4 events were rare, 0.3%. Median time to onset was 25 days (range, 1 to 630 days), and median time to improvement to grade 1 or less was 33 days (Janssen Pharmaceuticals, 2023).
Use of an over-the-counter emollient moisturizer may be recommended to help prevent or manage mild skin-related toxicities. Ammonium lactate cream may also be effective (Mancia et al., 2021). In more severe cases, topical corticosteroids or dermatology consult may be required (Narayan et al., 2022).
Nail
Talquetamab may cause a variety of nail-related disorders, including nail discoloration, thinning, ridging, breaking, or loss over time. These events occurred in 50% of patients. Patients experienced koilonychia, nail cuticle fissure, nail discoloration, ridging, and pitting.
Patients starting on talquetamab should be counseled to follow good hand hygiene, including keeping fingers and toes cleaned with nails trimmed, wearing comfortable shoes with extra room around the toes, avoiding nail polish (or use imitation fingernails), and wearing gloves for housecleaning and gardening to minimize nail damage and prevent infection. Over-the-counter moisturizers may also be useful in this setting, in addition to nail soaks, or in more severe cases topical steroids.
Oral and Mucosal
Oral-related adverse effects associated with talquetamab affected 80% of patients, with grade 3 toxicity in 2.1%. These included dysgeusia (49%), dry mouth (34%), dysphagia (23%), ageusia (18%), and decrease weight (62%). Median time to onset was 15 days (range, 1–634 days), and median duration to resolution to baseline was 43 days (range, 1–530 days). In 65% of patients, oral toxicity did not resolve to baseline. Weight loss occurred regardless of having oral toxicity: 29% of patients with grade 2 (10% or greater) and 2.7% of patients with grade 3 (20% or greater) weight loss. The median time to onset of grade 2 or higher was 67 days (range: 6–407 days) and a median time to resolution of 50 days (range of 1 to 403 days). In patients that reported weight loss, 57% did not resolve.
Initially, patients should be managed with mouth rinses, including salt water or steroid liquid formulations. If symptoms progress, nutrition consult and pain management strategies should be incorporated in an effort to prevent significant discomfort or weight loss. Finally, gastrointestinal or ear, nose, and throat consult may be recommended in severe cases.
Infections
Infections were common in the MonumenTAL-1 phase II trial with 16% of patients experiencing serious infections, 1.5% being fatal infections. 17% of patients had grade 3 or 4 infections, most common were bacteria (8%), including sepsis and COVID-19 (2.7%). It is recommended to follow institutional/local guidelines and consider administering prophylactic antimicrobials when managing patients on talquetamab. In severe cases, infectious disease should be consulted.
Elranatamab
Most recently, elranatamab was approved (under accelerated approval) for treatment of patients with RRMM who have received at least four prior lines of therapy, including an immunomodulatory agent, a proteasome inhibitor, and an anti-CD38 monoclonal antibody. Similarly to teclistamab, elranatamab targets both BCMA and CD3 antigens.
In the pivotal MagnetisMM-3 phase I/II trial, a total of 183 patients were treated, with 96.9% being triple-class refractory. The most common adverse reactions (> 20%) included CRS, fatigue, injection site reaction, diarrhea, upper respiratory infection, myalgias, pneumonia, reduced appetite, rash, cough, nausea, and fevers (Pfizer Inc., 2023). Injection site reactions with subcutaneous injections were common but typically resolved (Pfizer Inc., 2023). Elranatamab is therefore administered with premedications such as acetaminophen, dexamethasone, and diphenhydramine.
Patients should be hospitalized for 48 hours after administration of the first step-up dose and for 24 hours after the second step-up dose due to risk of CRS. In the MagnetisMM-3 trial, 58% of patients had CRS, with grade 1 CRS in 44%, grade 2 in 14%, and grade 3 in 0.5% (Figure 4). Thirteen percent of patients had recurrent CRS. Most patients (43%) had CRS after step-up dose 1. With step-up dose 2, 19% of patients had CRS, and 7% experienced CRS after the first treatment dose. Only 1.6% of patients had CRS with subsequent doses. The median time to onset of CRS was 2 days (range: 1 to 9 days) with a median duration of 2 days (range: 1 to 19 days; Pfizer Inc., 2023).

Figure 4. Elranatamab recommended dosing. Adapted from Pfizer Inc. (2023).
In the MagnetisMM-3 trial, neurologic toxicity occurred in 59% of patients, with grade 3/4 neurotoxicity in 7%. The most common neurologic adverse events included headache (18%), encephalopathy (15%), motor dysfunction (13%), sensory neuropathy (13%) and Guillain-Barre Syndrome (0.5%). ICANS occurred in 3.3% of patients at the recommended treatment dose; however, most patients developed ICANS after step-up dose 1 (2.7%). One patient had ICANS after step-up dose 2, and 1 patient had ICANS with subsequent doses. Recurrent ICANS occurred in 1.1% of patients. The median time to ICANS onset was 3 days (range: 1 to 4 days), with a median duration of 2 days (range: 1 to 18 days). ICANS most frequently presented with depressed level of consciousness and grade 1/2 ICE scores (Pfizer Inc., 2023). Due to risk of CRS and ICANS, elranatamab is only available through a REMS program.
Infections
In the MagnetisMM-3 trial, 42% of patients had serious infections, including opportunistic infections, with 31% experiencing grade 3/4 infections and 7% fatal infections. The most common serious infections (≥ 5%) were pneumonia and sepsis. Therefore, patients should be closely monitored for fevers, cough, and other symptoms of infections. While there is currently no standard of care for use of prophylactic antimicrobials and antivirals with elranatamab, individual institutional guidelines should be followed. In patients with hypogammaglobulinemia, it is recommended to administer IVIG when appropriate (Pfizer Inc., 2023).
Hepatotoxicity
Due to risk of hepatotoxicity, it is important to monitor for related symptoms including fatigue, anorexia, right upper abdominal discomfort, dark urine, and jaundice. Liver enzymes should be closely monitored prior to and during administration of elranatamab. In the MagnetisMM-3 trial, liver enzyme elevations occurred with or without concurrent CRS. Elevated ALT occurred in 36% of patients and 40% had elevated AST. Total bilirubin elevations were much less common, occurring in only 0.5% of patients (Pfizer Inc., 2023).
Long-Term Adverse Events With Bispecific Antibodies
While the long-term adverse events of BsAbs are largely unknown, hypogammaglobulinemia, pancytopenia, and risk of infections are likely to be common long-term toxicities in patients receiving BsAbs. As more novel therapies continue to develop and become standard practice, the need for frequent monitoring is essential. There are currently no guidelines on revaccinations, but it may be worth checking patients’ antibody titers 4 to 5 months post-initiation of BsAb therapy to assess the need for revaccination due to possible B-cell aplasia and increased immune suppression.
Conclusion
As described in this article, BsAbs are associated with a variety of severe adverse events; however, risk can be significantly reduced with appropriate patient education, adverse event recognition, and timely management. During the treatment initiation and step-up dosing phase, advanced practitioners should monitor closely for signs and symptoms of CRS and ICANS as well as hepatotoxicity. As patients continue treatment in the outpatient setting, monitoring of other adverse events, including cytopenias and infection, becomes more prudent. Finally, patients should receive education prior to treatment initiation on the unique adverse events associated with BsAbs that may impact their quality of life, in addition to strategies for adverse event prevention and management. A multidisciplinary team approach is imperative in patient care and coordination during BsAb treatment.
Acknowledgment
Writing assistance was provided by Larry Rosenberg, PhD.
Disclosure
Dr. Faiman has served as a consultant for Amgen, BMS, Janssen, and Pfizer. Dr. Rice has served on the advisory board for Janssen. Ms. Mistry has no conflict of interest to disclose.
References
Ayuketang, F. A., & Jäger, U. (2022). Management of Cytokine Release Syndrome (CRS) and HLH. In: N. Kröger, J. Gribben, C. Chabannon, et al. (Eds). The EBMT/EHA CAR-T Cell Handbook [Internet]. Cham (CH): Springer; 2022. Chapter 26. https://doi.org/10.1007/978-3-030-94353-0_26
Buelow, B., Choudry, P., Clarke, S., Dang, K., Davison, L., Aldred, S. F.,…Schooten, W. V. (2018). Pre-clinical development of TNB-383B, a fully human T-cell engaging bispecific antibody targeting BCMA for the treatment of multiple myeloma. Journal of Clinical Oncology, 36(suppl), 8034–8034
Chari, A., Minnema, M. C., Berdeja, J. G., Oriol, A., van de Donk, N. W. C. J., Rodríguez-Otero, P.,…Krishnan, A. (2022). Talquetamab, a T-cell-redirecting GPRC5D bispecific antibody for multiple myeloma. New England Journal of Medicine, 387(24), 2232–2244. https://doi.org/10.1056/NEJMoa2204591
Cosenza, M., Sacchi, S., & Pozzi, S. (2021). Cytokine release syndrome associated with T-cell-based therapies for hematological malignancies: Pathophysiology, clinical presentation, and treatment. International Journal of Molecular Sciences, 22(14), 7652. https://doi.org/10.3390/ijms22147652
Csizmar, C. M., & Ansell, S. M. (2021). Engaging the innate and adaptive antitumor immune response in lymphoma. International Journal of Molecular Sciences, 22(7), 3302. https://doi.org/10.3390/ijms22073302
Esfandiari, A., Cassidy, S., & Webster, R. M. (2022). Bispecific antibodies in oncology. Nature Reviews. Drug Discovery, 21(6), 411–412. https://doi.org/10.1038/d41573-022-00040-2
Hua, G., Scanlan, R., Straining, R., & Carlson, D. S. (2023). Teclistamab-cqyv: The first bispecific T-cell engager antibody for the treatment of patients with relapsed or refractory multiple myeloma. Journal of the Advanced Practitioner in Oncology, 14(2), 163–171. https://doi.org/10.6004/jadpro.2023.14.2.7
Janssen Pharmaceuticals. (2022). Tecvayli (teclistamab-cqyv) package insert. https://www.janssenlabels.com/package-insert/product-monograph/prescribing-information/TECVAYLI-pi.pdf
Janssen Pharmaceuticals. (2023). Talvey (talquetamab-tgvs) package insert. https://www.janssenlabels.com/package-insert/product-monograph/prescribing-information/TALVEY-pi.pdf
Janakiram, M., & Krishnan, A. (2023). Bispecific antibodies in refractory multiple myeloma: Basics and unanswered questions. ASCO Daily News. https://dailynews.ascopubs.org/do/bispecific-antibodies-refractory-multiple-myeloma-basics-and-unanswered-questions
Kumar, S., D'Souza, A., Shah, N., Rodriguez, C., Voorhees, P. M., Orlando, F.,…Vij, R. (2021). A phase 1 first-in-human study of Tnb-383B, a BCMA x CD3 bispecific T-cell redirecting antibody, in patients with relapsed/refractory multiple myeloma. Blood, 138(suppl 1), 900. https://doi.org/10.1182/blood-2021-150757
Labrijn, A. F., Janmaat, M. L., Reichert, J. M., & Parren, P. W. H. I. (2019). Bispecific antibodies: a mechanistic review of the pipeline. Nature Reviews. Drug Discovery, 18(8), 585–608. https://doi.org/10.1038/s41573-019-0028-1
Le, R. Q., Li, L., Yuan, W., Shord, S. S., Nie, L., Habtemariam, B. A.,…Pazdur, R. (2018). FDA approval summary: Tocilizumab for treatment of chimeric antigen receptor T cell-induced severe or life-threatening cytokine release syndrome. Oncologist, 23(8), 943–947. https://doi.org/10.1634/theoncologist.2018-0028
Lee, D. W., Santomasso, B. D., Locke, F. L., Ghobadi, A., Turtle, C. J., Brudno, J. N.,…Neelapu, S. S. (2019). ASTCT consensus grading for cytokine release syndrome and neurologic toxicity associated with immune effector cells. Biology of Blood and Marrow Transplantation: Journal of the American Society for Blood and Marrow Transplantation, 25(4), 625–638. https://doi.org/10.1016/j.bbmt.2018.12.758
Lee, H. C., Bumma, N., Richter, J. R., Dhodapkar, M. V., Hoffman, J. E., Suvannasankha, A.,…Jagannath, S. (2023). LINKER-MM1 study: Linvoseltamab (REGN5458) in patients with relapsed/refractory multiple myeloma. Journal of Clinical Oncology, 16(suppl), 8006–8006.
Lesokhin, A. M., Richter, J., Trudel, S., Cohen A. D., Spencer, A., Forsberg, P. A.,…Harrison, S. J. (2022). Enduring responses after 1-year, fixed-duration cevostamab therapy in patients with relapsed/refractory multiple myeloma: Early experience from a phase I study. Blood, 140(suppl 1), 4415–4417. https://doi.org/10.1182/blood-2022-157547
Mancia, S. S., Farrell, A., Louw, K., Florendo, E., Aronson, E., Purcell, K.,…Chari, A. (2021). Characterization and management of oral and dermatological toxicities in patients receiving the CD3 X GPRC5D bispecific antibody talquetamab (JNJ-64407564) for the treatment of relapsed and/or refractory multiple myeloma. Poster presentation at the annual American Society of Hematology meeting. Blood, 138(suppl 1), 1658. https://doi.org/10.1182/blood-2021-153817
Martin, T. G., Mateos, M. V., Nooka, A., Banerjee, A., Kobos, R., Pei, L.,…Rodriguez, C. (2023). Detailed overview of incidence and management of cytokine release syndrome observed with teclistamab in the MajesTEC-1 study of patients with relapsed/refractory multiple myeloma. Cancer, 129(13), 2035–2046. https://doi.org/10.1002/cncr.34756
Mohan, M., Nagavally, S., Dhakal, B., Radhakrishnan, S. V., Chhabra, S., D'Souza, A., & Hari, P. (2022). Risk of infections with B-cell maturation antigen-directed immunotherapy in multiple myeloma. Blood Advances, 6(8), 2466–2470. https://doi.org/10.1182/bloodadvances.2021006178
Moreau, P., Garfall, A. L., van de Donk, N. W. C. J., Nahi, H., San-Miguel, J. F., Oriol, A.,… Usmani, S. Z. (2022). Teclistamab in relapsed or refractory multiple myeloma. New England Journal of Medicine, 387(6), 495–505. https://doi.org/10.1056/NEJMoa2203478
Neelapu, S. S. (2019). Managing the toxicities of CAR T-cell therapy. Hematological Oncology, 37(S1), 48–52. https://doi.org/10.1002/hon.2595
Pfizer Inc. (2023). Elrexfio (elranatamab) package insert. https://labeling.pfizer.com/ShowLabeling.aspx?id=19669
Rees, J. H. Management of immune effector cell-associated neurotoxicity syndrome (ICANS). (2022). In: Kröger, N., Gribben, J., Chabannon C, Yakoub-Agha, I., & Einsele, H. (Eds.). The EBMT/EHA CAR-T Cell Handbook [Internet], Chp. 27. https://www.ebmt.org/ebmteha-car-t-cell-handbook
Shalabi, H., Sachdev, V., Kulshreshtha, A., Cohen, J. W., Yates, B., Rosing, D. R., Sidenko, S., Delbrook, C., Mackall, C., Wiley, B., Lee, D. W., & Shah, N. N. (2020). Impact of cytokine release syndrome on cardiac function following CD19 CAR-T cell therapy in children and young adults with hematological malignancies. Journal for Immunotherapy of Cancer, 8(2), e001159. https://doi.org/10.1136/jitc-2020-001159
Siegler, E. L., & Kenderian, S. S. (2020). Neurotoxicity and cytokine release syndrome after chimeric antigen receptor T cell therapy: Insights into mechanisms and novel therapies. Frontiers in Immunology, 11, 1973. https://doi.org/10.3389/fimmu.2020.01973
Smith, L., & Venella, K. (2017). Cytokine release syndrome: Inpatient care for side effects of CAR T-cell therapy. Clinical Journal of Oncology Nursing. CJON, 21(2), 29–34. https://doi.org/10.1188/17.CJON.S2.29-34
Trudel, S., Bahlis, N., Spencer, A., Kaedbey, R., Otero, P. R., Harrison, S. J.,…Mateos, M.-V. (2022). Pretreatment with tocilizumab prior to the CD3 bispecific cevostamab in patients with relapsed/refractory multiple myeloma (RRMM) showed a marked reduction in cytokine release syndrome incidence and severity. Blood, 140(suppl 1), 1363–1365.https://ashpublications.org/blood/article/140/Supplement%201/1363/491397/Pretreatment-with-Tocilizumab-Prior-to-the-CD3
Verkleij, C. P. M., Broekmans, M. E. C., van Duin, M., Frerichs, K. A., Kuiper, R., de Jonge, A. V.,…van de Donk, N. W. C. J. (2021). Preclinical activity and determinants of response of the GPRC5DxCD3 bispecific antibody talquetamab in multiple myeloma. Blood Advances, 5(8), 2196–2215. https://doi.org/10.1182/bloodadvances.2020003805
Waldman, A. D., Fritz, J. M., & Lenardo, M. J. (2020). A guide to cancer immunotherapy: from T cell basic science to clinical practice. Nature Reviews. Immunology, 20(11), 651–668. https://doi.org/10.1038/s41577-020-0306-5