Patient With Debilitating Bone Pain Related to Myelofibrosis
Presentation
RR is a 61-year-old female with hyperthyroidism, depression, migraines, and post-essential thrombocythemia myelofibrosis (post-ET MF) with progression to acute myeloid leukemia (AML).
She was diagnosed with CALR-positive ET in 2006 and was successfully managed without the development of any thrombotic or hemorrhagic complications. Unfortunately, in January 2020, she developed anemia, leukocytosis, and progressive splenomegaly. A repeat bone marrow biopsy was performed, confirming suspected disease transformation from ET to myelofibrosis (MF). She was started on ruxolitinib, which did improve the leukocytosis and reduce her spleen size.
At the time of transformation, RR was also experiencing severe diffuse bilateral leg pain with peripheral paresthesias. The pain was so intense that she required a wheelchair for her clinic visits. Ruxolitinib did not seem to help with this pain. Although bone pain is a commonly reported symptom in patients with MF, this degree of bone pain warranted further investigation.
Workup
RR was evaluated with a number of imaging studies including x-ray, MRI of the spine and bilateral lower extremities, and CT scan of the bilateral lower extremities. The MRI reports did mention diffuse low signal intensity of the bone marrow, a common finding in MF. No etiology for her pain was identified, and importantly, there was no evidence of a mass, infection, or occult fracture.
RR was referred to neurology and rheumatology for complete workup as well; labs and further diagnostic studies were unrevealing. A number of pain regimens were trialed. While some provided relief, the positive effects were transient. She continued to functionally decline.
Progression to AML
In May 2020, RR developed worsening leukocytosis, thrombocytopenia, and peripheral blasts up to 15%. Another bone marrow biopsy was performed and revealed progression from MF to AML with 30% blasts in the bone marrow. She had acquired mutations in ASXL1 and TET2 and monosomy 7 [del(7q)] on cytogenetic analysis.
Many options were discussed with RR, ranging from induction chemotherapy and transplant to pursuing palliative care in light of her current performance status. She decided to pursue treatment with azacitidine plus venetoclax, with stem cell transplant as the goal. She did achieve a morphologic leukemia-free state and proceeded to matched unrelated donor stem cell transplant.
Post-Transplant
RR did have a complicated hospital stay post-transplant with acute graft-versus-host disease and infections, which have resolved. She had delayed engraftment—a common experience in this patient population—but has recently achieved transfusion independence. She no longer suffers from bone pain and is fully ambulatory. She does work with physical therapy due to weakness that developed as a result of many months of immobility.
Discussion
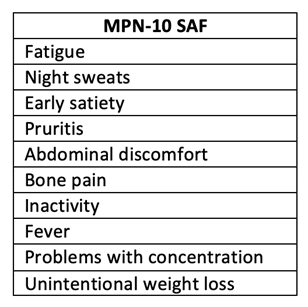
Bone pain is reported in 44% of patients with MF.1 As advanced practice providers, we assess our patients’ symptoms on a regular basis and should be familiar with those related to an underlying myeloproliferative neoplasm (MPN). The most experienced symptoms are outlined in the MPN-Symptom Assessment Form (MPN-SAF) and the MPN-10, which is a more concise list of symptoms1 and should be implemented into routine clinical practice.
Bone pain related to an underlying ET or even low-risk MF would not be in and of itself a reason to pursue stem cell transplant. Indications for transplant in this patient population involve a number of disease-related features in high-risk MF and post-MF AML. In the case of this patient who required a stem cell transplant due to disease progression to AML, resolution of pain was an apparent benefit. After thorough pre-transplant evaluation for alternative etiologies, this resolution confirmed our suspicion that this was related to the underlying MPN. It is important to provide appropriate workup any time symptoms seem out of proportion to what you would anticipate for your patient given their underlying hematologic malignancy.
Reference
- Mesa RA, et al. The Myelofibrosis Symptom Assessment Form (MFSAF): an evidence-based brief inventory to measure quality of life and symptomatic response to treatment in myelofibrosis. Leuk Res. 2009;33:1199-1203.