Prophylactic Tocilizumab in Selected High-Risk or Outpatient CAR-T Populations
Presentation
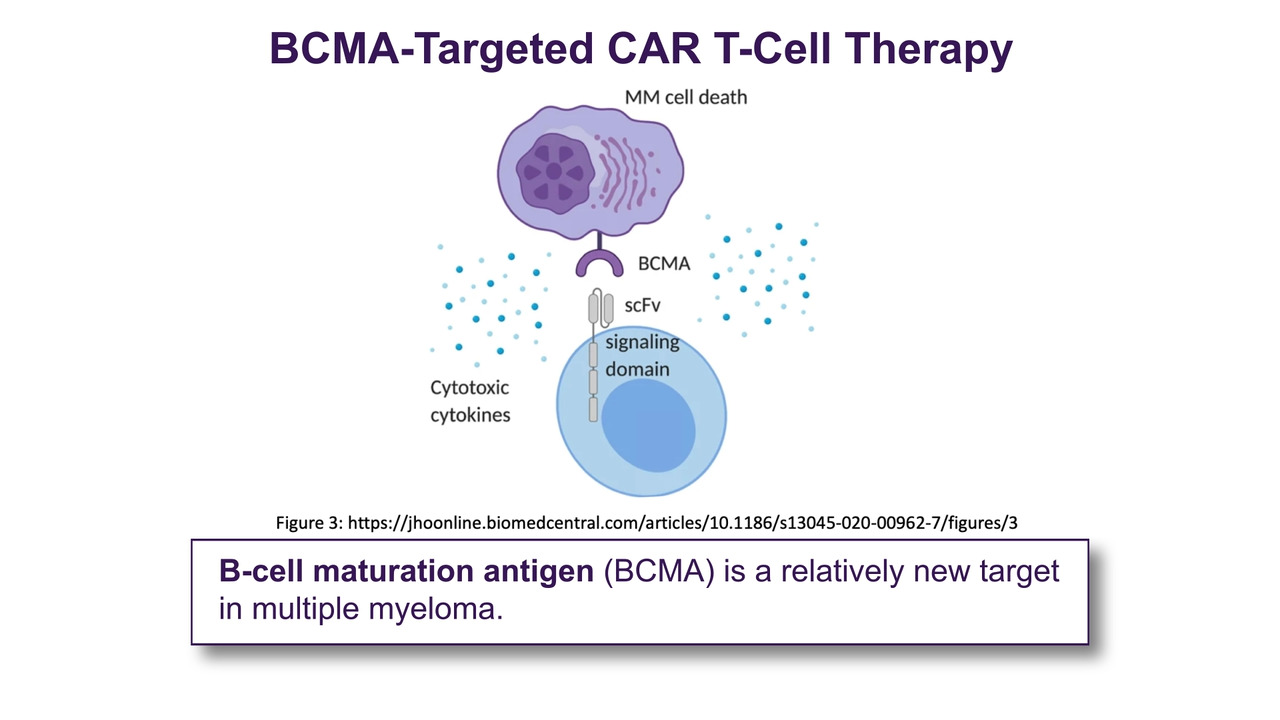
A 68-year-old male with relapsed/refractory IgG kappa multiple myeloma presented for B-cell maturation antigen (BCMA)–directed CAR T-cell therapy after disease progression through four prior lines of therapy, including a proteasome inhibitor, an immunomodulatory agent, and an anti-CD38 monoclonal antibody. His disease was refractory to his most recent regimen.
Given his age, high disease burden at lymphodepletion, and the institutional transition to an outpatient CAR T-cell delivery model, the multidisciplinary cellular therapy team elected to administer prophylactic tocilizumab to mitigate the risk of cytokine release syndrome (CRS).
The patient underwent lymphodepleting chemotherapy with fludarabine (30 mg/m² IV daily for 3 days) and cyclophosphamide (300 mg/m² IV daily for 3 days) prior to receiving BCMA-directed CAR T-cell infusion with ciltacabtagene autoleucel. Per institutional protocol informed by emerging outpatient data, the patient received prophylactic tocilizumab 8 mg/kg IV approximately 1 hour after CAR T-cell infusion.
Workup, Clinical Course, and Management
The patient’s vital signs prior to infusion were stable.
Vital Signs on Day 0 (Infusion Day)
|
Vital Sign |
Value |
|
Blood pressure |
128/78 mm Hg |
|
Heart rate |
82 beats per minute |
|
Respiratory rate |
16 breaths per minute |
|
Temperature |
98.6° F |
|
Peripheral oxygen saturation |
98% on room air |
The patient tolerated infusion without immediate reaction. Tocilizumab 8 mg/kg IV was administered prophylactically within 1 hour of CAR T infusion.
On Day 2, the patient developed a low-grade fever (100.5°F).
Vital Signs on Day 2
|
Vital Sign |
Value |
|
Blood pressure |
118/74 mm Hg |
|
Heart rate |
92 beats per minute |
|
Respiratory rate |
18 breaths per minute |
|
Temperature |
100.5° F |
|
Peripheral oxygen saturation |
97% on room air |
An infectious workup (blood cultures, urinalysis, and chest imaging) was negative. The patient was non-neutropenic. Acetaminophen was administered, with symptomatic improvement. No hypotension or hypoxia developed. The patient’s immune effector cell-associated encephalopathy (ICE) score remained 10/10. The patient was monitored for 6 hours in clinic and returned to local lodging with a caregiver after no additional vital sign changes.
Day 3 and Beyond
The patient’s fever had resolved. The patient remained hemodynamically stable and was managed entirely in the outpatient setting without hospitalization.
The patient’s ICE score remained a 10/10 throughout the remainder of the 14-day monitoring period, and no immune effector cell-associated neurotoxicity syndrome (ICANS) developed.
Discussion
CRS is the most common toxicity associated with CAR T-cell therapy and results from rapid immune activation and cytokine production, particularly interleukin-6 (IL-6).1 The hallmark symptom of CRS is fever. Severity is graded based on the presence of hypotension and/or hypoxia.2
BCMA-directed CAR T-cell therapies such as ciltacabtagene autoleucel have demonstrated high response rates in relapsed/refractory multiple myeloma but are associated with high rates of CRS in clinical trials.3Historically, CRS incidence has exceeded 80% in pivotal studies, although most events were grade 1–2.
Tocilizumab, an IL-6 receptor antagonist, is U.S. Food and Drug Administration approved for the treatment (not prevention) of CAR-T–associated CRS. Traditionally, it is administered reactively for grade ≥ 2 CRS. However, emerging data suggest that prophylactic administration may reduce the incidence or severity of CRS without compromising CAR-T efficacy.4,5
A recent outpatient study of idecabtagene vicleucel demonstrated reduced rates of CRS and no ICANS in patients receiving prophylactic tocilizumab compared with historical controls.6,7Similar exploratory analyses presented in 2025 suggest that early IL-6 blockade may blunt peak cytokine signaling while preserving CAR T expansion.4
In this case, prophylactic tocilizumab was associated with:
- Development of only grade 1 CRS
- No hypotension or hypoxia
- No ICANS
- Successful outpatient management
- No need for additional IL-6 blockade
Although this represents a single-patient experience, it aligns with emerging evidence supporting prophylactic strategies in selected high-risk or outpatient CAR-T populations.
Clinical Pearls
- Fever remains the earliest and most consistent sign of CRS, although in the setting of prophylactic tocilizumab, institutions may err on the side of more aggressive management of hypotension and hypoxia without fever in patients post CAR T-cell therapy.
- Prophylactic tocilizumab may reduce progression to higher-grade CRS.
- Early IL-6 blockade has not yet demonstrated impairment of CAR-T efficacy in retrospective analyses.
- Prophylaxis may be particularly valuable in outpatient CAR-T programs.
- Prospective randomized data are still needed to define optimal timing and patient selection.
References
- National Cancer Institute. CAR T Cells: Engineering Patients’ Immune Cells to Treat Their Cancers. Accessed February 25, 2026. https://www.cancer.gov/about-cancer/treatment/research/car-t-cells.
- Lee DW, Santomasso BD, Lockeet FL, al. ASTCT consensus grading for cytokine release syndrome and neurologic toxicity associated with immune effector cells. Biol Blood Marrow Transplant. 2019;25(4):625-638.
- Chaudhary N, Roy S, Lin CF, et al. Real-world incidence, characteristics and management of cytokine release syndrome induced by chimeric antigen receptor T-cell therapy across hematologic malignancies. Presented at: American Society of Hematology Annual Meeting; December 9-12, 2023; San Diego, CA. Abstract 5150.
- Gavriilaki M, Evangelidis P, Evangelidis N, Dolgyras P, Sakellari I, Gavriilaki E. Tocilizumab prophylaxis in patients receiving CAR-T cell immunotherapy for hematological malignancies: a systematic review and meta-analysis. Blood. 2025;146(suppl 1):7668. doi:10.1182/blood-2025-7668.
- Kowalski A, Lykon J, Diamond B, et al. Tocilizumab prophylaxis for patients with multiple myeloma treated with bispecific antibodies. Blood Adv. 2025;9(19):4979-4986. doi:10.1182/bloodadvances.2025016911.
- Peres E, Farhan S, Emole J, Abidi MH, Alavi A, Peres C. Tocilizumab prophylaxis following idecabtagene vicleucel in the outpatient setting in patients with relapsed or refractory multiple myeloma. Transplant Cell Ther. 2026;32(2):S201-S202.
- Patel A, Parekh D, Desai D, Olojakpoke E, Khan A, Kumar PA. Mitigating CRS in CAR-T therapy: real-world outcomes of prophylactic tocilizumab administration. Clin Lymphoma Myeloma Leuk. 2025;25(suppl 1):S1052. doi:10.1016/S2152-2650(25)02849-6.