Hemophagocytic Lymphohistiocytosis Following CAR T-Cell Therapy in a Patient With Multiple Myeloma
Patient Presentation
A 48-year-old male patient with a history of IgA kappa multiple myeloma presented with disease progression following multiple lines of therapy including cyclophosphamide, bortezomib, and dexamethasone (CyBorD); daratumumab plus lenalidomide, bortezomib, and dexamethasone (Dara+RVD); autologous stem cell transplant (ASCT); and consolidation. The patient was evaluated for CAR T-cell therapy due to progression at day 180 post-ASCT.
Initial Workup, Diagnosis, and Staging
The bone marrow biopsy prior to CAR T-cell therapy revealed 90% plasma cells and cytopenia.1 Stem cells were collected in case a stem cell boost was needed. The patient was monitored closely for toxicity during bridging therapy with carfilzomib, cyclophosphamide, and dexamethasone.
The primary diagnosis was IgA kappa multiple myeloma with cytogenetic abnormalities (1p1q), classifying this as high-risk disease.1 Disease progression was noted post consolidation therapy.
Treatment Plan
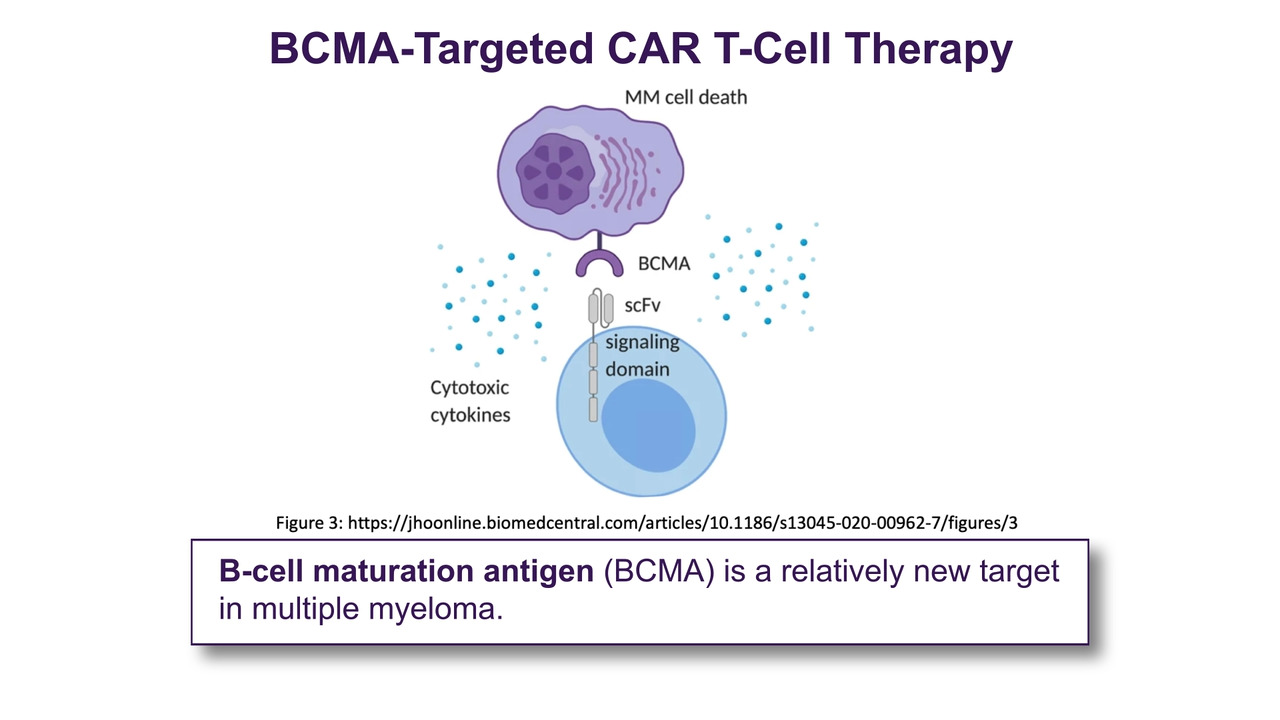
CAR T-cell therapy with ciltacabtagene autoleucel was administered following bridging therapy with fludarabine and cyclophosphamide. The patient experienced cytokine release syndrome (CRS), which was managed with tocilizumab and dexamethasone. On day 7 post-infusion, concern for hemophagocytic lymphohistiocytosis (HLH) prompted initiation of anakinra and dexamethasone. A bone marrow biopsy showed markedly hypocellular marrow with fibrosis and hemophagocytosis.2,3
Timeline of Treatment Milestones

ASCT, autologous stem cell transplant; CRS, cytokine release syndrome; CyBorD, cyclophosphamide, bortezomib, and dexamethasone; Dara + RVD, daratumumab plus lenalidomide, bortezomib, and dexamethasone; ICANS, immune effector cell-associated neurotoxicity syndrome; HLH, hemophagocytic lymphohistiocytosis.
HLH was suspected based on clinical findings including elevated ferritin (10,612 ng/mL), lactate dehydrogenase (7,494 U/L), and interleukin-2 receptor levels (8,392 pg/mL). A bone marrow biopsy confirmed hemophagocytosis. Treatment included 200 mg of anakinra every 8 hours and a dexamethasone taper over 10 days. CRS and immune effector cell–associated neurotoxicity syndrome (ICANS) scores remained at 0 following intervention.
CRS/ICANS Grading and Interventions

The AP’s Role
Advanced practitioners (APs) play a key role in monitoring for CRS and HLH, initiating timely interventions, coordinating transfusions, managing neutropenia, and educating the patient on immunosuppressive precautions, risk for infections and other complications, and post-transplant immunizations.
HLH is a rare but serious complication of CAR T-cell therapy requiring prompt recognition and treatment. APs are critical in identifying early signs of toxicity and coordinating multidisciplinary care. Furthermore, immune effector cell–associated hemophagocytic lymphohistiocytosis-like syndrome (IEC-HS) is a rare but potentially fatal complication following CAR T-cell therapy and T-cell engager antibody treatments for non-Hodgkin lymphoma and relapsed/refractory multiple myeloma. IEC-HS is characterized by symptoms such as cytopenia, coagulopathy, elevated liver enzymes, and hyperferritinemia.
Hines and colleagues analyzed 15,852 adverse events from the FDA Adverse Event Reporting System, identifying 263 IEC-HS cases (1.7%). Tisagenlecleucel and axicabtagene ciloleucel (axi-cel) had the highest incidence of IEC-HS. Mortality among patients with IEC-HS was high (58.1%), with axi-cel and teclistamab showing the highest associated death rates. IEC-HS often co-occurred with CRS and ICANS.4
This case study highlights the importance of ongoing monitoring and supportive care in patients post-CAR T-cell therapy. It also illustrates the complexity of managing relapsed multiple myeloma and the potential for HLH following CAR T-cell therapy. Advanced practitioners are essential in recognizing complications, initiating treatment, and supporting patients through intensive therapies.5-7

References
- Rajkumar SV. Multiple myeloma: 2024 update on diagnosis, risk-stratification, and treatment. American Journal of Hematology. 2024;99(9):1802–1824. doi:10.1002/ajh.27422
- Rasche L, Hudecek M, Einsele H. CAR T-cell therapy in multiple myeloma: Mission accomplished? Blood. 2024;143(4):305-310. doi:10.1182/blood.2023021221
- Swan D, Madduri D, Hocking J. CAR T-cell therapy in multiple myeloma: Current status and future challenges. Blood Cancer J. 2024;14(1):206. doi:10.1038/s41408-024-01191-8
- Hines MR, Knight TE, McNerney KO, et al. Immune effector cell-associated hemophagocytic lymphohistiocytosis–like syndrome. Transplantation and Cellular Therapy. 2023;29(7):438.e1-438.e16. doi:10.1016/j.jtct.2023.03.006
- Meeths M, Bryceson YT. Genetics and pathophysiology of haemophagocytic lymphohistiocytosis. Acta Paediatrica. 2021;110(12):3271-3280. doi:10.1111/apa.16013
- Allen CE, McClain KL. Pathophysiology and epidemiology of hemophagocytic lymphohistiocytosis. American Society of Hematology. Education Program. 2015;2015(1):177-182. doi:10.1182/asheducation-2015.1.177
- Chandrakasan S, Filipovich AH. Hemophagocytic lymphohistiocytosis: Advances in pathophysiology and treatment. Journal of Pediatrics. 2013;163(2):316-320. Accessed August 25, 2025. http://www.hlhsupport.org/uploads/1/4/5/6/14569950/jpeds2013chandrakasan.pdf
Resources
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Multiple Myeloma. Version 2.2025. Published 2024. Accessed August 18, 2025. https://www.nccn.org/professionals/physician_gls/pdf/myeloma.pdf
- Myeloma Australia. Clinical Practice Guideline: Multiple Myeloma. Myeloma Australia; 2022. Accessed August 18, 2025. https://myeloma.org.au/wp-content/uploads/2022/09/MSAG_Myeloma-Clinical-Practice-Guideline-2022_Final-1.pdf
- Nadeem O. An update on CAR T-cell therapy in multiple myeloma. Dana-Farber Cancer Institute. Published 2025. Accessed August 18, 2025. https://www.dana-farber.org/for-physicians/clinical-resources/hematologic-malignancies/advances-newsletter/2025-issue-20/multiple-myeloma-cart-t-cell-therapy-update