A Rare Instance of Testicular Relapse of T-Cell Acute Lymphoblastic Leukemia
Presentation
A 56-year-old male in remission from T-cell acute lymphoblastic leukemia (T-ALL), presents to an urgent care center with unilateral testicular enlargement with mild tenderness. His T-ALL treatment history includes therapy with hyper-CVAD + nelarabine, vincristine and dexamethasone (MOAD) x 2 for eradication of minimal residual disease (MRD), and an allogenic matched unrelated donor hematopoietic stem cell transplant (allo-HSCT) 11 years ago. During his urgent care visit, a testicular ultrasound was suggestive of epididymitis. He was treated with a 10-day course of ciprofloxacin without improvement in swelling and pain. He returned to urgent care and underwent a repeat testicular ultrasound showing concerns for infiltration by neoplasm. He was then further evaluated by his hematologist/oncologist and found to have a 7-8 cm enlarged left testicle significantly stretching the scrotal tissue resulting in erythema.
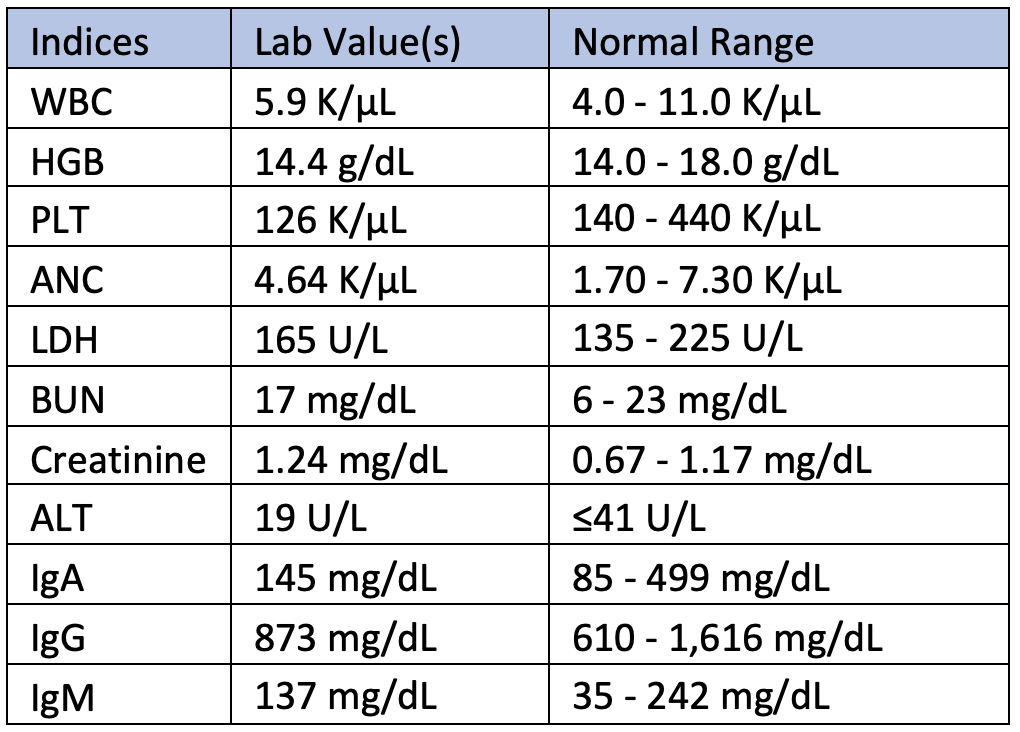
Lab Values
Workup
- Testicular ultrasound with Doppler: Heterogeneous echotexture measuring 5 x 4 x 4 cm with increased vascular flow.
- Bone marrow aspiration/biopsy: Normocellular (30-40%) marrow with trilineage hematopoiesis. Diploid male karyotype. Flow cytometry positive for minimal residual disease (MRD) at 0.13%.
- Radical orchiectomy: Near early T-cell precursor ALL involving the testis, peri-testicular soft tissue, and epididymis with somatic mutations in JAK3-A573V, NOTCH1-Q2394, and FGFR3-S53R.
- PET/CT: Performed after orchiectomy due to insurance restrictions. Nodular focus of soft tissue with mild FDG uptake in the left external iliac region.
Diagnosis
Near early T-cell precursor ALL (near-ETP ALL) by radical orchiectomy with MRD present in the bone marrow.
Treatment
The patient was treated with systemic combination chemotherapy of hyper-CVAD (cyclophosphamide, vincristine, doxorubicin hydrochloride, dexamethasone) + venetoclax and intrathecal (IT) cytarabine alternating with IT methotrexate, and then received radiation to contralateral testis and scrotum (200 cGy in 12 fractions).
Management
The patient underwent routine labs 1-2 times weekly to monitor for transfusion requirements. A treatment plan was created for continued chemotherapy with consolidation (4-8 cycles) and 2 lumbar punctures per cycle with IT chemotherapy (to total 8), followed by a second allogeneic HSCT.
Discussion
The testicles and central nervous system (CNS) are recognized as immunological sanctuary sites for leukemic cells due to the physiologic blood-brain and blood-testes barrier. This case highlights a rare occurrence of leukemic relapse following a prolonged remission in an adult patient with T-ALL who had previously undergone allogeneic HSCT. Testicular relapse of ALL can clinically resemble common urological infections, such as epididymo-orchitis, or even a primary testicular neoplasm. However, it is crucial to maintain a high level of suspicion for leukemic involvement in patients with a history of leukemia, regardless of the time elapsed since diagnosis or prior treatment.
The reduced incidence of extramedullary relapse can be attributed to the introduction of high-dose methotrexate, optimization of CNS-directed prophylactic therapy through intrathecal (IT) chemotherapy as the standard of care, and overall improvements in systemic chemotherapy regimens.1-3 These advancements in the treatment of acute lymphoblastic leukemia have virtually eliminated the need for prophylactic craniospinal irradiation to the CNS and local irradiation or orchiectomy for testicular involvement.
The timing of relapse, the involvement of additional relapse sites, and the cytogenetic and molecular profile of the relapsed disease are key factors in determining the most appropriate treatment strategy for testicular relapses. Molecular and genetic diagnostics also offer valuable insights into risk assessment and prognosis, further informing treatment decisions.4
Ultimately, the approach for management should integrate a multidisciplinary team approach to include hematology-oncology, urology, and radiation oncology.
Further Directions
CAR-T therapy provides a novel therapeutic strategy for relapsed ALL. Research substantiates that CAR-T cells hold the potential to migrate into the sanctuary sites of the central nervous system and the testes, and thus, its use in these settings may have positive implications on the prognosis for such patients.5-7 The evidence for the efficacy of CAR T-cell therapy for T-ALL has yet to be substantiated; however, advances in the development of CD5- and CD7-engineered CAR-T cells may possess great potential for treatment, especially in the relapsed-refractory setting for these patients.
References
- Gao RW, Dusenbery KE, Cao Q, Smith AR, Yuan J. Augmenting total body irradiation with a cranial boost before stem cell transplantation protects against post-transplant central nervous system relapse in acute lymphoblastic leukemia. Biol Blood Marrow Transplant. 2018;24(3):501-506. doi:10.1016/j.bbmt.2017.11.013
- Hijiya N, Liu W, Sandlund JT, et al. Overt testicular disease at diagnosis of childhood acute lymphoblastic leukemia: lack of therapeutic role of local irradiation. Leukemia. 2005;19(8):1399-1403. doi:10.1038/sj.leu.2403843
- Sirvent N, Suciu S, Bertrand Y, Uyttebroeck A, Lescoeur B, Otten J. Overt testicular disease (OTD) at diagnosis is not associated with a poor prognosis in childhood acute lymphoblastic leukemia: results of the EORTC CLG Study 58881. Pediatr Blood Cancer. 2007;49(3):344-348. doi:10.1002/pbc.20716
- Nguyen HTK, Terao MA, Green DM, Pui CH, Inaba H. Testicular involvement of acute lymphoblastic leukemia in children and adolescents: Diagnosis, biology, and management. Cancer. 2021;127(17):3067-3081. doi:10.1002/cncr.33609
- Mohty M, Gautier J, Malard F, et al. CD19 chimeric antigen receptor-T cells in B-cell leukemia and lymphoma: current status and perspectives. Leukemia. 2019;33(12):2767-2778. doi:10.1038/s41375-019-0615-5
- Yu J, Hu Y, Pu C, et al. Successful chimeric Ag receptor modified T cell therapy for isolated testicular relapse after hematopoietic cell transplantation in an acute lymphoblastic leukemia patient. Bone Marrow Transplant. Jul 2017;52(7):1065-1067. doi:10.1038/bmt.2017.64
- Rubinstein JD, Krupski C, Nelson AS, O'Brien MM, Davies SM, Phillips CL. Chimeric antigen receptor T cell therapy in patients with multiply relapsed or refractory extramedullary leukemia. Biol Blood Marrow Transplant. 2020;26(11):e280-e285. doi:10.1016/j.bbmt.2020.07.036